UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT
REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): September 26, 2023
TALARIS THERAPEUTICS, INC.
(Exact name of registrant as specified in its charter)
|
|
|
|
|
| Delaware |
|
001-40384 |
|
83-2377352 |
| (State or other jurisdiction
of incorporation) |
|
(Commission
File Number) |
|
(I.R.S. Employer
Identification No.) |
|
|
|
| 93 Worcester St.
Wellesley, Massachusetts |
|
02481 |
| (Address of principal executive offices) |
|
(Zip Code) |
Registrant’s telephone number, including area code: (502)
398-9250
Check the appropriate box below
if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| ☒ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ☐ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17
CFR 240.14a-12) |
| ☐ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ☐ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
|
|
|
|
|
| Title of each class |
|
Trade
Symbol(s) |
|
Name of each exchange
on which registered |
| Series A Common Stock, $0.0001 par value per share |
|
TALS |
|
The Nasdaq Global Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of
1933 (§ 230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§ 240.12b-2 of this chapter).
Emerging growth company ☒
If an emerging growth
company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
| Item 7.01 |
Regulation FD Disclosure |
As previously announced, on June 22, 2023, Talaris Therapeutics, Inc., a Delaware corporation (“Talaris”), Terrain Merger Sub, Inc., a Delaware
corporation and a wholly owned subsidiary of Talaris (“Merger Sub”), and Tourmaline Bio, Inc., a Delaware corporation (“Tourmaline”), entered into an Agreement and Plan of Merger (the “Merger Agreement”), pursuant to
which, among other matters, and subject to the satisfaction or waiver of the conditions set forth in the Merger Agreement, Merger Sub will merge with and into Tourmaline, with Tourmaline continuing as a wholly owned subsidiary of Talaris and the
surviving corporation of the merger (the “Merger”).
On September 26, 2023, Tourmaline updated information reflected in an investor
presentation, which is attached as Exhibit 99.1 to this Current Report on Form 8-K and is incorporated herein by reference. Representatives of Tourmaline will use the updated presentation in various meetings
with investors and analysts from time to time.
The information in Item 7.01 of this Current Report on Form 8-K,
including the information set forth in Exhibit 99.1, is being furnished and shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), nor shall Exhibit
99.1 furnished herewith be deemed incorporated by reference in any filing under the Securities Act of 1933, as amended, or the Exchange Act, except as shall be expressly set forth by specific reference in such a filing.
Forward-Looking Statements
This Current Report on Form 8-K and the exhibit furnished herewith contain “forward-looking statements” within the meaning of the “safe harbor” provisions of the Private Securities Litigation Reform Act of 1995, including
but not limited to, express or implied statements regarding the structure, timing and completion of the proposed Merger; the combined company’s listing on Nasdaq after closing of the proposed Merger; expectations regarding the ownership
structure of the combined company; the anticipated timing of the closing of the Merger; each company’s and the combined company’s expected cash position at the closing of the proposed Merger and cash runway of the combined company; the
future operations of the combined company; the nature, strategy and focus of the combined company; the development and commercial potential and potential benefits of any product candidates or platform technologies of the combined company;
anticipated preclinical and clinical drug development activities and related timelines, including the expected timing for data and other clinical results; the competitive landscape of the combined company; anticipated intellectual property
timelines; and other statements that are not historical fact. All statements other than statements of historical fact contained in this Current Report on Form 8-K are forward-looking statements. These
forward-looking statements are made as of the date they were first issued, and were based on the then-current expectations, estimates, forecasts, and projections, as well as the beliefs and assumptions of management. There can be no assurance that
future developments affecting Talaris, Tourmaline or the proposed transaction will be those that have been anticipated.
Forward-looking statements are
subject to a number of risks and uncertainties, many of which involve factors or circumstances that are beyond Talaris’ control. Talaris’ actual results could differ materially from those stated or implied in forward-looking statements due
to a number of factors, including but not limited to (i) the risk that the conditions to the closing of the proposed Merger are not satisfied, including the failure to timely obtain shareholder approval for the transaction, if at all;
(ii) uncertainties as to the timing of the consummation of the proposed Merger and the ability of each of Talaris and Tourmaline to consummate the proposed Merger; (iii) risks related to Talaris’ ability to manage its operating
expenses and its expenses associated with the proposed Merger pending closing; (iv) risks related to the failure or delay in obtaining required approvals from any governmental or quasi-governmental entity necessary to consummate the proposed
Merger; (v) the risk that as a result of adjustments to the exchange ratio, Talaris shareholders and Tourmaline stockholders could own more or less of the combined company than is currently anticipated; (vi) risks related to the market
price of Talaris’ common stock relative to the value suggested by the exchange ratio; (vii) unexpected costs, charges or expenses resulting from the transaction; (viii) potential adverse reactions or changes to business relationships
resulting from the announcement or completion of the proposed Merger; (ix) the uncertainties associated with Tourmaline’s platform technologies, as well as risks associated with the clinical development and regulatory approval of product
candidates, including potential delays in the commencement, enrollment and completion of clinical trials; (x) risks related to the inability of the combined company to obtain sufficient additional capital to continue to advance these product
candidates and its preclinical programs; (xi) uncertainties in obtaining successful clinical results for product candidates and unexpected costs that may result therefrom; (xii) risks related to the failure to realize any value from
product candidates and preclinical
programs being developed and anticipated to be developed in light of inherent risks and difficulties involved in successfully bringing product candidates to market; (xiii) risks associated
with the possible failure to realize certain anticipated benefits of the proposed Merger, including with respect to future financial and operating results; (xiv) risks associated with Talaris’ financial close process; (xv) the risk
that the pre-closing financing is not consummated; and (xvi) the risk that Talaris shareholders receive more or less of the cash dividend than is currently anticipated, among others. Actual results and
the timing of events could differ materially from those anticipated in such forward-looking statements as a result of these risks and uncertainties. These and other risks and uncertainties are more fully described in periodic filings with the SEC,
including the factors described in the section titled “Risk Factors” in Talaris’ Annual Report on Form 10-K for the year ended December 31, 2022 filed with the SEC, and in other filings
that Talaris makes and will make with the SEC in connection with the proposed Merger, including the Proxy Statement described below under “Additional Information and Where to Find It.” You should not place undue reliance on these
forward-looking statements, which are made only as of the date hereof or as of the dates indicated in the forward-looking statements. Talaris expressly disclaims any obligation or undertaking to release publicly any updates or revisions to any
forward-looking statements contained herein to reflect any change in its expectations with regard thereto or any change in events, conditions or circumstances on which any such statements are based. This Current Report on Form 8-K does not purport to summarize all of the conditions, risks and other attributes of an investment in Talaris or Tourmaline.
Participants in the Solicitation
This Current Report on
Form 8-K and the exhibit filed or furnished herewith relate to the proposed merger transaction involving Talaris and Tourmaline and may be deemed to be solicitation material in respect of the proposed merger
transaction. In connection with the proposed merger transaction, Talaris has filed relevant materials with the SEC, including a registration statement on Form S-4 (the “Form
S-4”) that contains a proxy statement (the “Proxy Statement”) and prospectus. This Current Report on Form 8-K is not a substitute for the Form S-4, the Proxy Statement or for any other document that Talaris may file with the SEC and or send to Talaris’ shareholders in connection with the proposed merger transaction. BEFORE MAKING ANY VOTING DECISION,
INVESTORS AND SECURITY HOLDERS OF TALARIS ARE URGED TO READ THE FORM S-4, THE PROXY STATEMENT AND OTHER DOCUMENTS FILED WITH THE SEC CAREFULLY AND IN THEIR ENTIRETY WHEN THEY BECOME AVAILABLE BECAUSE THEY WILL
CONTAIN IMPORTANT INFORMATION ABOUT TALARIS, THE PROPOSED MERGER TRANSACTION AND RELATED MATTERS.
No Offer or Solicitation
This Current Report on Form 8-K and the exhibit furnished herewith do not constitute an offer to sell or the
solicitation of an offer to buy any securities nor a solicitation of any vote or approval with respect to the proposed transaction or otherwise. No offering of securities shall be made except by means of a prospectus meeting the requirements of
Section 10 of the U S. Securities Act of 1933, as amended, and otherwise in accordance with applicable law.
Additional Information and Where to
Find It
Investors and security holders may obtain free copies of the Form S-4, the Proxy Statement and other
documents filed by Talaris with the SEC through the website maintained by the SEC at http://www.sec.gov. Copies of the documents filed by Talaris with the SEC are also available free of charge on Talaris’ website at www.talaristx.com, or by
contacting Talaris’ Investor Relations at investors@talaristx.com. Talaris, Tourmaline, and their respective directors and certain of their executive officers may be considered participants in the solicitation of proxies from Talaris’
shareholders with respect to the proposed merger transaction under the rules of the SEC. Information about the directors and executive officers of Talaris is set forth in its Annual Report on Form 10-K for the
year ended December 31, 2022, which was filed with the SEC on March 31, 2023, and in subsequent documents filed with the SEC. Additional information regarding the persons who may be deemed participants in the proxy solicitations and a
description of their direct and indirect interests, by security holdings or otherwise, are also included in the Form S-4, the Proxy Statement and other relevant materials to be filed with the SEC when they
become available. You may obtain free copies of this document as described above.
| Item 9.01 |
Financial Statements and Exhibits |
(d) Exhibits
|
|
|
| Exhibit
No. |
|
Document |
|
|
| 99.1 |
|
Investor Presentation of Tourmaline Bio, Inc., dated September 26, 2023. |
|
|
| 104 |
|
Cover Page Interactive Data File (embedded within the Inline XBRL document). |
SIGNATURE
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned
hereunto duly authorized.
|
|
|
|
|
|
|
|
|
|
|
TALARIS THERAPEUTICS, INC. |
|
|
|
|
| Date: September 26, 2023 |
|
|
|
By: |
|
/s/ Mary Kay Fenton |
|
|
|
|
|
|
May Kay Fenton |
|
|
|
|
|
|
Chief Financial Officer and Interim Chief Financial Officer |
Exhibit 99.1 Sell-side Analyst Day September 26, 2023

Disclaimer This communication contains “forward-looking
statements” within the meaning of the “safe harbor” provisions of the Private Securities Litigation Reform Act of 1995, including but not limited to, express or implied statements regarding the structure, timing and completion of
the proposed Merger; the combined company’s listing on Nasdaq after closing of the proposed Merger; expectations regarding the ownership structure of the combined company; the anticipated timing of closing; each company’s and the
combined company’s expected cash position at the closing of the proposed Merger and cash runway of the combined company; the future operations of the combined company; the nature, strategy and focus of the combined company; the development and
commercial potential and potential benefits of TOUR006; anticipated preclinical and clinical drug development activities and related timelines, including the expected timing for data and other clinical results; the competitive landscape of the
combined company; anticipated intellectual property timelines; and other statements that are not historical fact. All statements other than statements of historical fact contained in this communication are forward-looking statements. These
forward-looking statements are made as of the date they were first issued, and were based on the then-current expectations, estimates, forecasts, and projections, as well as the beliefs and assumptions of management. Forward-looking statements are
subject to a number of risks and uncertainties, many of which involve factors or circumstances that are beyond Talaris’, Tourmaline’s or the combined company’s control. Actual results could differ materially from those stated or
implied in forward-looking statements due to a number of factors, including but not limited to (i) the risk that the conditions to the closing of the proposed Merger are not satisfied, including the failure to timely obtain shareholder approval for
the transaction, if at all; (ii) uncertainties as to the timing of the consummation of the proposed Merger and the ability of each of Talaris and Tourmaline to consummate the proposed Merger; (iii) risks related to Talaris’ ability to manage
its operating expenses and its expenses associated with the proposed merger pending closing; (iv) risks related to the failure or delay in obtaining required approvals from any governmental or quasi-governmental entity necessary to consummate the
proposed Merger; (v) the risk that as a result of adjustments to the exchange ratio, Talaris shareholders and Tourmaline stockholders could own more or less of the combined company than is currently anticipated; (vi) risks related to the market
price of Talaris’ common stock relative to the value suggested by the exchange ratio; (vii) unexpected costs, charges or expenses resulting from the transaction; (viii) potential adverse reactions or changes to business relationships resulting
from the announcement or completion of the proposed Merger; (ix) the uncertainties associated with Tourmaline’s platform technologies, as well as risks associated with the clinical development and regulatory approval of product candidates,
including potential delays in the commencement, enrollment and completion of clinical trials; (x) risks related to the inability of the combined company to obtain sufficient additional capital to continue to advance these product candidates and its
preclinical programs; (xi) uncertainties in obtaining successful clinical results for product candidates and unexpected costs that may result therefrom; (xii) risks related to the failure to realize any value from product candidates and preclinical
programs being developed and anticipated to be developed in light of inherent risks and difficulties involved in successfully bringing product candidates to market; (xiii) risks associated with the possible failure to realize certain anticipated
benefits of the proposed Merger, including with respect to future financial and operating results; (xiv) risks associated with Talaris’ financial close process; (xv) the risk that the pre-closing financing is not consummated; and (xvi) the
risk that Talaris shareholders receive more or less of the cash dividend than is currently anticipated, among others. Actual results and the timing of events could differ materially from those anticipated in such forward- looking statements as a
result of these risks and uncertainties. These and other risks and uncertainties are more fully described in filings that Talaris makes and will make with the SEC in connection with the proposed Merger, including the Proxy Statement described below
under “Additional Information and Where to Find It.” You should not place undue reliance on these forward-looking statements, which are made only as of the date hereof or as of the dates indicated in the forward-looking statements.
Talaris, Tourmaline and the combined company expressly disclaims any obligation or undertaking to release publicly any updates or revisions to any forward-looking statements contained herein to reflect any change in its expectations with regard
thereto or any change in events, conditions or circumstances on which any such statements are based. Tourmaline obtained the industry, market and competitive position data used throughout this presentation from its own internal estimates and
research, as well as from industry and general publications, and research, surveys and studies conducted by third parties. Internal estimates are derived from publicly available information released by industry analysts and third-party sources,
Tourmaline’s internal research and its industry experience, and are based on assumptions made by Tourmaline based on such data and its knowledge of the industry and market, which it believes to be reasonable. In addition, while Tourmaline
believes the industry, market and competitive position data included in this presentation is reliable and based on reasonable assumptions, Tourmaline has not independently verified any third-party information, and all such data involve risks and
uncertainties and are subject to change based on various factors. This presentation contains trademarks, services marks, trade names and copyrights of Tourmaline and other companies, which are the property of their respective owners. The use or
display of third parties’ trademarks, service marks, trade name or products in this presentation is not intended to, and does not imply, a relationship with Tourmaline, or an endorsement of sponsorship by Tourmaline. Solely for convenience,
the trademarks, service marks and trade names referred to in this presentation may appear with the ®, TM or SM symbols, but such references are not intended to indicate, in any way, that the company will not assert, to the fullest extent under
applicable law, their rights or the right of the applicable licensor to these trademarks, service marks and trade name. 2
Disclaimer (continued) Participants in the Solicitation This
communication relates to the proposed merger transaction involving Talaris and Tourmaline and may be deemed to be solicitation material in respect of the proposed merger transaction. In connection with the proposed merger transaction, Talaris has
filed relevant materials with the U.S. Securities and Exchange Commission (the “SEC”), including a registration statement on Form S-4 (the “Form S-4”) that contains a proxy statement (the “Proxy Statement”) and
prospectus. This communication is not a substitute for the Form S-4, the Proxy Statement or for any other document that Talaris may file with the SEC and or send to Talaris’ shareholders in connection with the proposed merger transaction.
BEFORE MAKING ANY VOTING DECISION, INVESTORS AND SECURITY HOLDERS OF TALARIS ARE URGED TO READ THE FORM S-4, THE PROXY STATEMENT AND OTHER DOCUMENTS FILED WITH THE SEC CAREFULLY AND IN THEIR ENTIRETY WHEN THEY BECOME AVAILABLE BECAUSE THEY WILL
CONTAIN IMPORTANT INFORMATION ABOUT TALARIS, THE PROPOSED MERGER TRANSACTION AND RELATED MATTERS. Additional Information and Where to Find It Investors and security holders may obtain free copies of the Form S-4, the Proxy Statement and other
documents filed by Talaris with the SEC through the website maintained by the SEC at http://www.sec.gov. Copies of the documents filed by Talaris with the SEC are also available free of charge on Talaris’ website at www.talaristx.com, or by
contacting Talaris’ Investor Relations at investors@talaristx.com. Talaris, Tourmaline, and their respective directors and certain of their executive officers may be considered participants in the solicitation of proxies from Talaris’
shareholders with respect to the proposed merger transaction under the rules of the SEC. Information about the directors and executive officers of Talaris is set forth in its Annual Report on Form 10-K for the year ended December 31, 2022, which was
filed with the SEC on March 31, 2023, and in subsequent documents filed with the SEC. Additional information regarding the persons who may be deemed participants in the proxy solicitations and a description of their direct and indirect interests, by
security holdings or otherwise, are also included in the Form S-4, the Proxy Statement and other relevant materials to be filed with the SEC when they become available. You may obtain free copies of this document as described above. No Offer or
Solicitation This communication does not constitute an offer to sell or the solicitation of an offer to buy any securities nor a solicitation of any vote or approval with respect to the proposed transaction or otherwise. No offering of securities
shall be made except by means of a prospectus meeting the requirements of Section 10 of the U S. Securities Act of 1933, as amended, and otherwise in accordance with applicable law. 3
Agenda 2:00 – 2:05 pm Introducing our team 2:05 – 2:20 pm
IL-6 renaissance 2:20 – 3:00 pm TED 3:00 – 3:40 pm ASCVD 3:40 – 3:50 pm Key business items 3:50 – 4:30 pm Q&A and discussion 4

Experienced leadership team Sandeep Kulkarni, MD Yung Chyung, MD Brad
Middlekauff, JD Susan Dana Jones, PhD Chief Technology Co-founder and Chief Medical Chief Business Officer and Chief Executive Officer Officer General Counsel Officer Kevin Johnson, PhD Ryan Iarrobino Gerhard Hagn Dora Rau Chief Regulatory Senior
Vice President, Senior Vice President, Senior Vice President, Officer Product Development Head of Commercial & BD Head of Quality 5
Key highlights An IL-6 renaissance is underway: new insights emerging
about a broad range of indications where IL-6 may be clinically validated TOUR006 offers potential for low volume, infrequent subcutaneous administration We are rapidly advancing TOUR006 into mid/late-stage development Our team has extensive
experience developing and commercializing antibodies for orphan and autoimmune diseases Cash runway expected to fund development through 2026* *Upon completion of the merger with Talaris and pre-closing financing 6
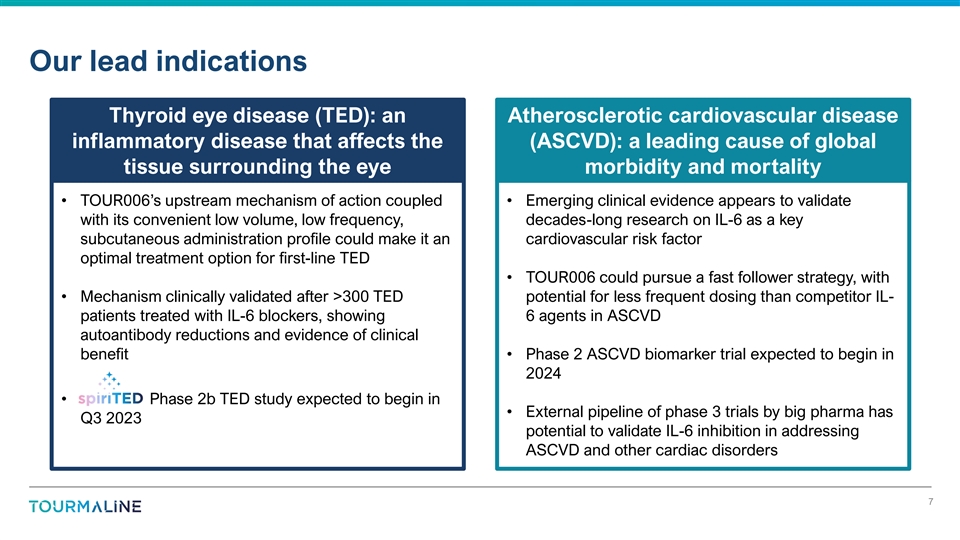
Our lead indications Thyroid eye disease (TED): an Atherosclerotic
cardiovascular disease inflammatory disease that affects the (ASCVD): a leading cause of global tissue surrounding the eye morbidity and mortality • TOUR006’s upstream mechanism of action coupled • Emerging clinical evidence
appears to validate with its convenient low volume, low frequency, decades-long research on IL-6 as a key subcutaneous administration profile could make it an cardiovascular risk factor optimal treatment option for first-line TED • TOUR006
could pursue a fast follower strategy, with • Mechanism clinically validated after >300 TED potential for less frequent dosing than competitor IL- patients treated with IL-6 blockers, showing 6 agents in ASCVD autoantibody reductions and
evidence of clinical benefit • Phase 2 ASCVD biomarker trial expected to begin in 2024 • Phase 2b TED study expected to begin in • External pipeline of phase 3 trials by big pharma has Q3 2023 potential to validate IL-6 inhibition
in addressing ASCVD and other cardiac disorders 7
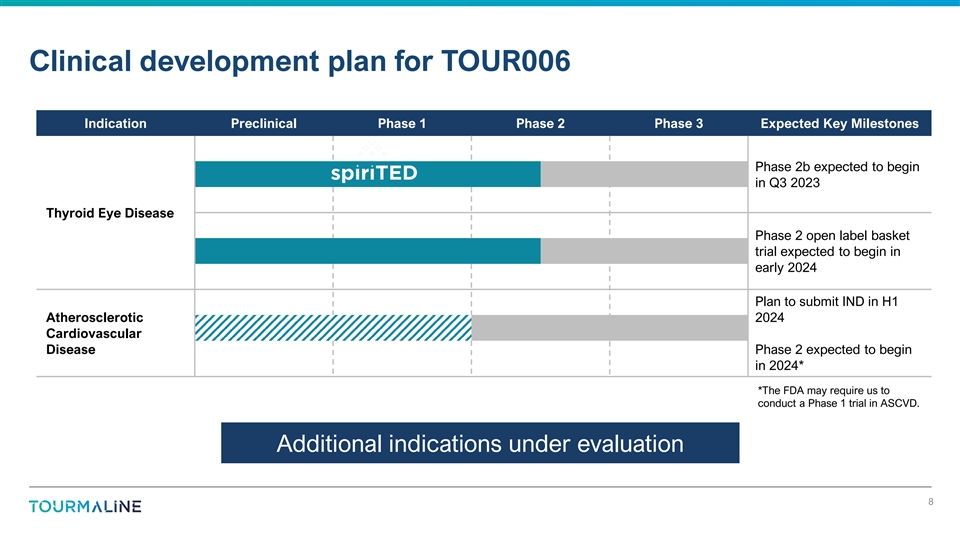
Clinical development plan for TOUR006 Indication Preclinical Phase 1
Phase 2 Phase 3 Expected Key Milestones Phase 2b expected to begin in Q3 2023 Thyroid Eye Disease Phase 2 open label basket trial expected to begin in early 2024 Plan to submit IND in H1 Atherosclerotic 2024 Cardiovascular Disease Phase 2 expected
to begin in 2024* *The FDA may require us to conduct a Phase 1 trial in ASCVD. Additional indications under evaluation 8
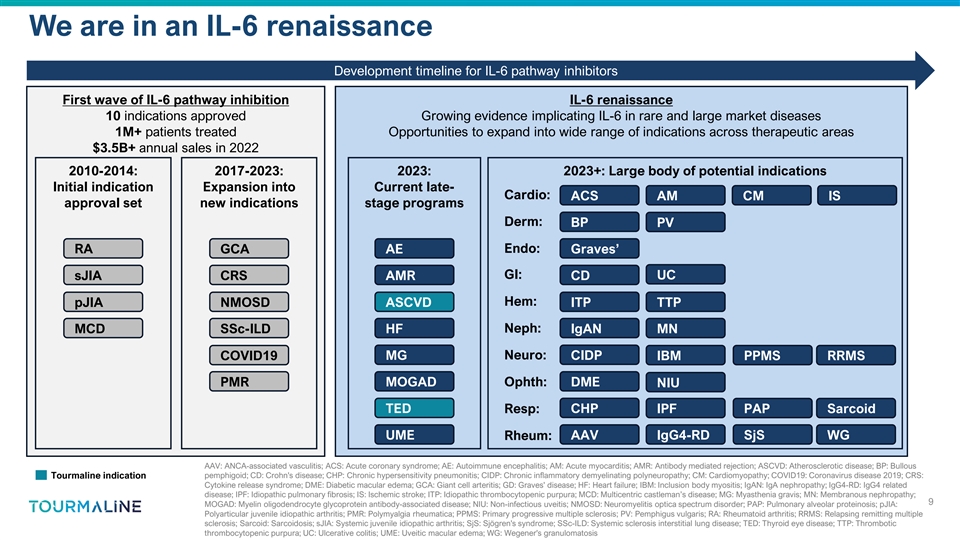
We are in an IL-6 renaissance Development timeline for IL-6 pathway
inhibitors First wave of IL-6 pathway inhibition IL-6 renaissance 10 indications approved Growing evidence implicating IL-6 in rare and large market diseases 1M+ patients treated Opportunities to expand into wide range of indications across
therapeutic areas $3.5B+ annual sales in 2022 2010-2014: 2017-2023: 2023: 2023+: Large body of potential indications Initial indication Expansion into Current late- Cardio: ACS AM CM IS approval set new indications stage programs Derm: BP PV RA GCA
AE Endo: Graves’ GI: sJIA CRS AMR CD UC pJIA NMOSD ASCVD Hem: ITP TTP MCD SSc-ILD HF Neph: IgAN MN COVID19 MG Neuro: CIDP IBM PPMS RRMS PMR MOGAD Ophth: DME NIU TED Resp: CHP IPF PAP Sarcoid UME Rheum: AAV IgG4-RD SjS WG AAV: ANCA-associated
vasculitis; ACS: Acute coronary syndrome; AE: Autoimmune encephalitis; AM: Acute myocarditis; AMR: Antibody mediated rejection; ASCVD: Atherosclerotic disease; BP: Bullous Tourmaline indication pemphigoid; CD: Crohn's disease; CHP: Chronic
hypersensitivity pneumonitis; CIDP: Chronic inflammatory demyelinating polyneuropathy; CM: Cardiomyopathy; COVID19: Coronavirus disease 2019; CRS: Cytokine release syndrome; DME: Diabetic macular edema; GCA: Giant cell arteritis; GD: Graves'
disease; HF: Heart failure; IBM: Inclusion body myositis; IgAN: IgA nephropathy; IgG4-RD: IgG4 related disease; IPF: Idiopathic pulmonary fibrosis; IS: Ischemic stroke; ITP: Idiopathic thrombocytopenic purpura; MCD: Multicentric castleman’s
disease; MG: Myasthenia gravis; MN: Membranous nephropathy; 9 MOGAD: Myelin oligodendrocyte glycoprotein antibody-associated disease; NIU: Non-infectious uveitis; NMOSD: Neuromyelitis optica spectrum disorder; PAP: Pulmonary alveolar proteinosis;
pJIA: Polyarticular juvenile idiopathic arthritis; PMR: Polymyalgia rheumatica; PPMS: Primary progressive multiple sclerosis; PV: Pemphigus vulgaris; RA: Rheumatoid arthritis; RRMS: Relapsing remitting multiple sclerosis; Sarcoid: Sarcoidosis; sJIA:
Systemic juvenile idiopathic arthritis; SjS: Sjögren's syndrome; SSc-ILD: Systemic sclerosis interstitial lung disease; TED: Thyroid eye disease; TTP: Thrombotic thrombocytopenic purpura; UC: Ulcerative colitis; UME: Uveitic macular edema; WG:
Wegener's granulomatosis
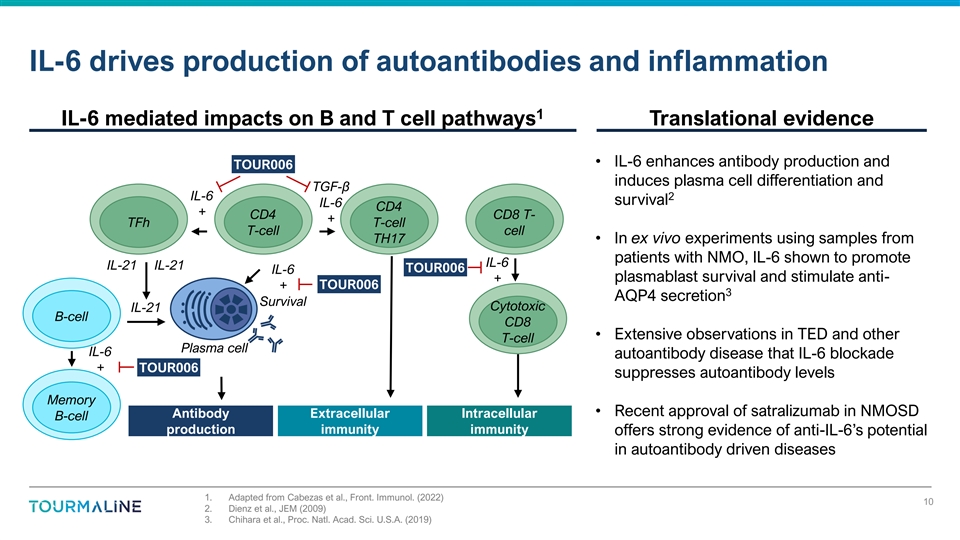
IL-6 drives production of autoantibodies and inflammation 1 IL-6
mediated impacts on B and T cell pathways Translational evidence • IL-6 enhances antibody production and TOUR006 induces plasma cell differentiation and TGF-β IL-6 2 survival IL-6 CD4 + CD4 CD8 T- + TFh T-cell T-cell cell TH17 • In
ex vivo experiments using samples from patients with NMO, IL-6 shown to promote IL-6 IL-21 IL-21 TOUR006 IL-6 + plasmablast survival and stimulate anti- TOUR006 + 3 AQP4 secretion Survival Cytotoxic IL-21 B-cell CD8 • Extensive observations in
TED and other T-cell Plasma cell IL-6 autoantibody disease that IL-6 blockade + TOUR006 suppresses autoantibody levels Memory • Recent approval of satralizumab in NMOSD Antibody Extracellular Intracellular B-cell production immunity immunity
offers strong evidence of anti-IL-6’s potential in autoantibody driven diseases 1. Adapted from Cabezas et al., Front. Immunol. (2022) 10 2. Dienz et al., JEM (2009) 3. Chihara et al., Proc. Natl. Acad. Sci. U.S.A. (2019)
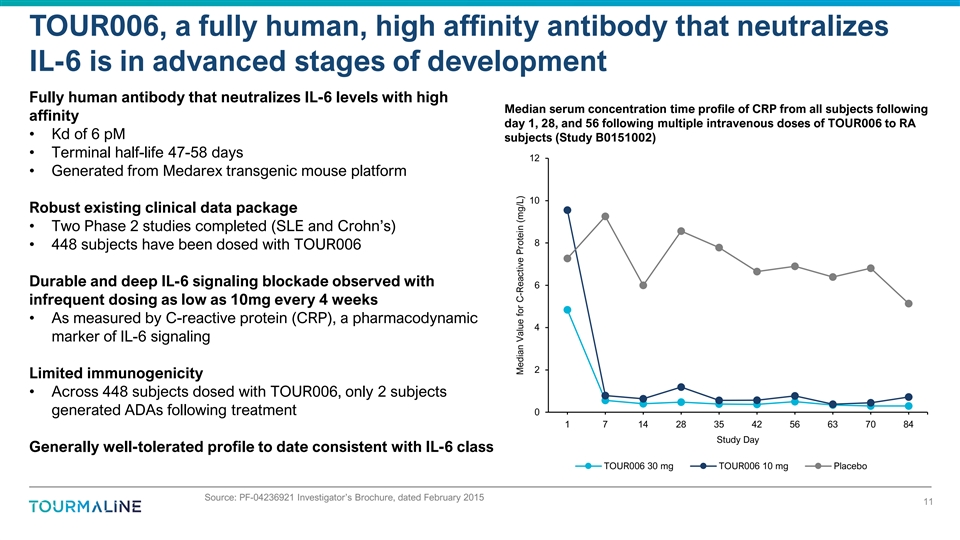
TOUR006, a fully human, high affinity antibody that neutralizes IL-6 is
in advanced stages of development Fully human antibody that neutralizes IL-6 levels with high Median serum concentration time profile of CRP from all subjects following affinity day 1, 28, and 56 following multiple intravenous doses of TOUR006 to RA
• Kd of 6 pM subjects (Study B0151002) • Terminal half-life 47-58 days 12 • Generated from Medarex transgenic mouse platform 10 Robust existing clinical data package • Two Phase 2 studies completed (SLE and Crohn’s) 8
• 448 subjects have been dosed with TOUR006 Durable and deep IL-6 signaling blockade observed with 6 infrequent dosing as low as 10mg every 4 weeks • As measured by C-reactive protein (CRP), a pharmacodynamic 4 marker of IL-6 signaling 2
Limited immunogenicity • Across 448 subjects dosed with TOUR006, only 2 subjects generated ADAs following treatment 0 1 7 14 28 35 42 56 63 70 84 Study Day Generally well-tolerated profile to date consistent with IL-6 class TOUR006 30 mg
TOUR006 10 mg Placebo Source: PF-04236921 Investigator’s Brochure, dated February 2015 11 Median Value for C-Reactive Protein (mg/L)
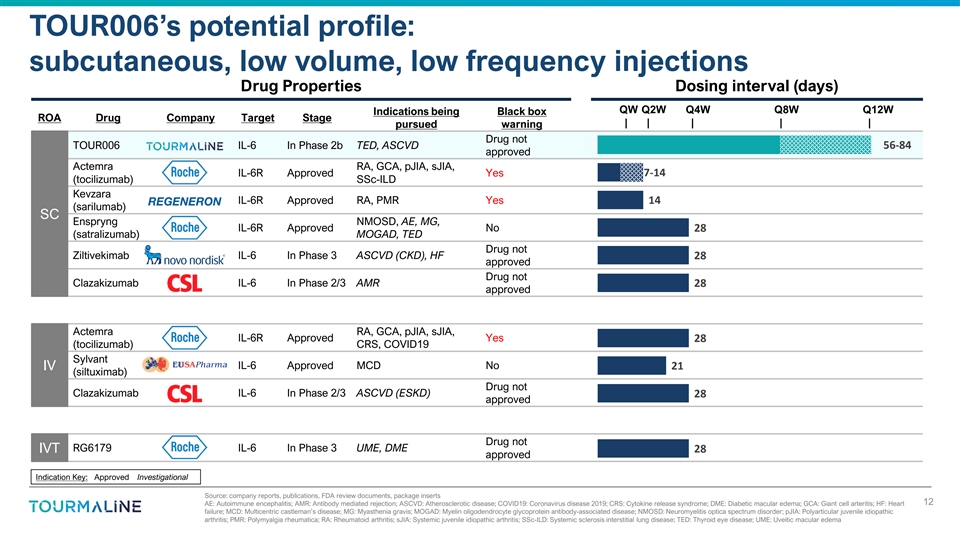
TOUR006’s potential profile: subcutaneous, low volume, low
frequency injections Drug Properties Dosing interval (days) QW Q2W Q4W Q8W Q12W Indications being Black box ROA Drug Company Target Stage | | | | | pursued warning Drug not TOUR006 IL-6 In Phase 2b TED, ASCVD 56-84 approved Actemra RA, GCA, pJIA,
sJIA, 7-14 IL-6R Approved Yes (tocilizumab) SSc-ILD Kevzara IL-6R Approved RA, PMR Yes 14 (sarilumab) SC Enspryng NMOSD, AE, MG, IL-6R Approved No 28 (satralizumab) MOGAD, TED Drug not Ziltivekimab IL-6 In Phase 3 ASCVD (CKD), HF 28 approved Drug
not Clazakizumab IL-6 In Phase 2/3 AMR 28 approved Actemra RA, GCA, pJIA, sJIA, IL-6R Approved Yes 28 (tocilizumab) CRS, COVID19 Sylvant IL-6 Approved MCD No 21 IV (siltuximab) Drug not Clazakizumab IL-6 In Phase 2/3 ASCVD (ESKD) 28 approved Drug
not RG6179 IL-6 In Phase 3 UME, DME IVT 28 approved Indication Key: Approved Investigational Source: company reports, publications, FDA review documents, package inserts 12 AE: Autoimmune encephalitis; AMR: Antibody mediated rejection; ASCVD:
Atherosclerotic disease; COVID19: Coronavirus disease 2019; CRS: Cytokine release syndrome; DME: Diabetic macular edema; GCA: Giant cell arteritis; HF: Heart failure; MCD: Multicentric castleman’s disease; MG: Myasthenia gravis; MOGAD: Myelin
oligodendrocyte glycoprotein antibody-associated disease; NMOSD: Neuromyelitis optica spectrum disorder; pJIA: Polyarticular juvenile idiopathic arthritis; PMR: Polymyalgia rheumatica; RA: Rheumatoid arthritis; sJIA: Systemic juvenile idiopathic
arthritis; SSc-ILD: Systemic sclerosis interstitial lung disease; TED: Thyroid eye disease; UME: Uveitic macular edema
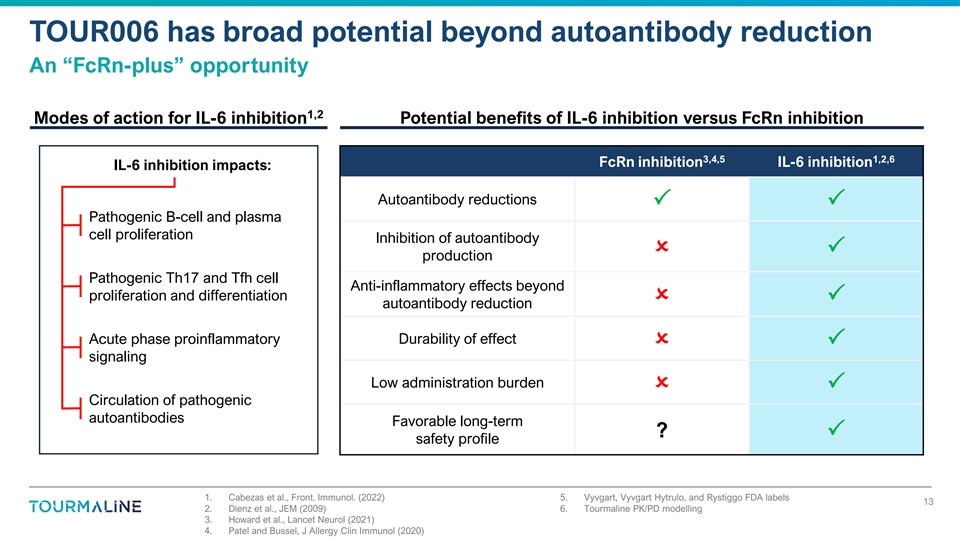
TOUR006 has broad potential beyond autoantibody reduction An
“FcRn-plus” opportunity 1,2 Modes of action for IL-6 inhibition Potential benefits of IL-6 inhibition versus FcRn inhibition 3,4,5 1,2,6 FcRn inhibition IL-6 inhibition IL-6 inhibition impacts: Autoantibody reductions PP
Pathogenic B-cell and plasma cell proliferation Inhibition of autoantibody OP production Pathogenic Th17 and Tfh cell Anti-inflammatory effects beyond proliferation and differentiation OP autoantibody reduction Acute phase
proinflammatory Durability of effect OP signaling Low administration burden OP Circulation of pathogenic autoantibodies Favorable long-term ? P safety profile 1. Cabezas et al., Front. Immunol. (2022) 5. Vyvgart, Vyvgart Hytrulo,
and Rystiggo FDA labels 13 2. Dienz et al., JEM (2009) 6. Tourmaline PK/PD modelling 3. Howard et al., Lancet Neurol (2021) 4. Patel and Bussel, J Allergy Clin Immunol (2020)
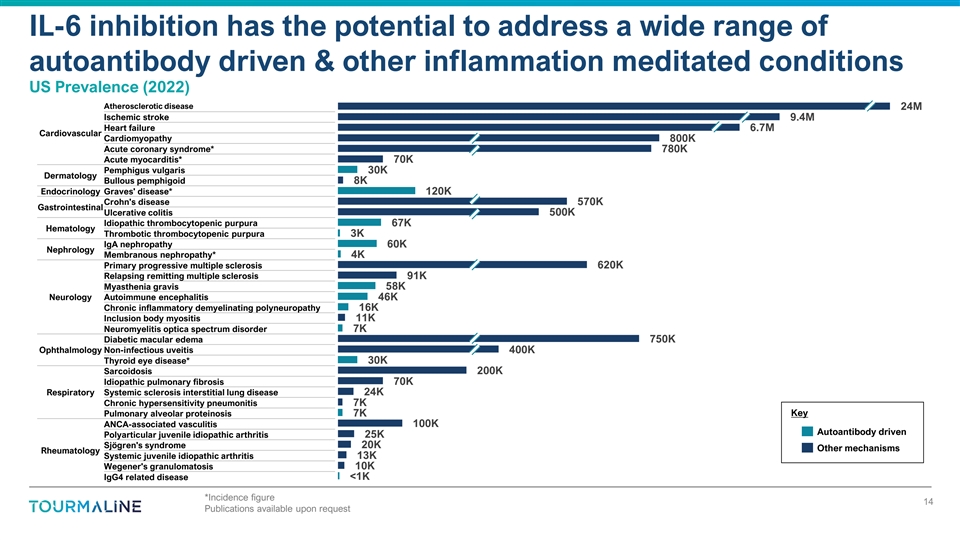
IL-6 inhibition has the potential to address a wide range of
autoantibody driven & other inflammation meditated conditions US Prevalence (2022) Atherosclerotic disease 24M Ischemic stroke 9.4M Heart failure 6.7M Cardiovascular Cardiomyopathy 800K Acute coronary syndrome* 780K Acute myocarditis* 70K
Pemphigus vulgaris 30K Dermatology Bullous pemphigoid 8K Endocrinology Graves' disease* 120K Crohn's disease 570K Gastrointestinal Ulcerative colitis 500K Idiopathic thrombocytopenic purpura 67K Hematology Thrombotic thrombocytopenic purpura 3K IgA
nephropathy 60K Nephrology Membranous nephropathy* 4K Primary progressive multiple sclerosis 620K Relapsing remitting multiple sclerosis 91K Myasthenia gravis 58K Neurology Autoimmune encephalitis 46K Chronic inflammatory demyelinating
polyneuropathy 16K Inclusion body myositis 11K Neuromyelitis optica spectrum disorder 7K Diabetic macular edema 750K Ophthalmology Non-infectious uveitis 400K Thyroid eye disease* 30K Sarcoidosis 200K Idiopathic pulmonary fibrosis 70K Respiratory
Systemic sclerosis interstitial lung disease 24K Chronic hypersensitivity pneumonitis 7K Key Pulmonary alveolar proteinosis 7K ANCA-associated vasculitis 100K Autoantibody driven 25K Polyarticular juvenile idiopathic arthritis Sjögren's
syndrome 20K Other mechanisms Rheumatology Systemic juvenile idiopathic arthritis 13K Wegener's granulomatosis 10K IgG4 related disease <1K *Incidence figure 14 Publications available upon request

Thyroid Eye Disease (TED)
Each year, TED impacts the lives of ~30k new patients in the US 1,2 at
an average age of ~45 Autoimmune disease associated with proliferation and damaging inflammation of the cell types surrounding the eye • Disfiguring symptoms that significantly affect QoL: proptosis, double-vision • Involvement of optic
nerve can be sight-threatening, requiring surgery We estimate up to 2/3 of the 30K new TED patients each year are 1,2 diagnosed as moderate-to-severe Pathophysiology driven by autoantibodies that bind to the TSH receptor, which is expressed on cell
types surrounding the eye • Same autoantibody can also cause Graves’ hyperthyroidism (GH); up to 3 95% of TED patients also have GH Source: Getty Images IL-6 is elevated in patients with TED and a growing body of evidence 4 suggests a
role in disease pathogenesis 1. Lazarus, Best Pract. Res. Clin. Endocrinol. Metab. (2012) 16 2. Bartalena et al., Front. Endocrinol. (2020) 3. Sabini et al., Eur. Thyroid J. (2018) 4. Hiromatsu et al., J. Clin. Endocrinol. Metab. (2000); Slowik et
al., Endocr. Res. (2012); Jyonouchi et al., Thyroid (2001); Hwang et al., Invest Ophthalmol Vis Sci (2009)
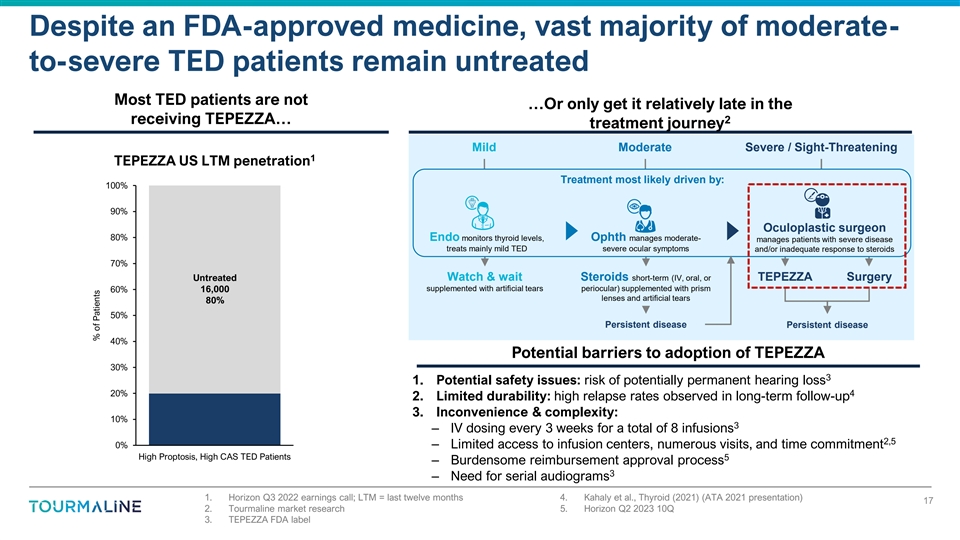
Despite an FDA-approved medicine, vast majority of moderate- to-severe
TED patients remain untreated Most TED patients are not …Or only get it relatively late in the receiving TEPEZZA… 2 treatment journey Mild Moderate Severe / Sight-Threatening 1 TEPEZZA US LTM penetration Treatment most likely driven by:
100% 90% Oculoplastic surgeon 80% Endo monitors thyroid levels, Ophth manages moderate- manages patients with severe disease treats mainly mild TED severe ocular symptoms and/or inadequate response to steroids 70% Untreated Watch & wait Steroids
short-term (IV, oral, or TEPEZZA Surgery 60% 16,000 supplemented with artificial tears periocular) supplemented with prism lenses and artificial tears 80% 50% Persistent disease Persistent disease 40% Potential barriers to adoption of TEPEZZA 30% 3
1. Potential safety issues: risk of potentially permanent hearing loss 20% 4 2. Limited durability: high relapse rates observed in long-term follow-up 3. Inconvenience & complexity: 10% 3 – IV dosing every 3 weeks for a total of 8
infusions 2,5 0% – Limited access to infusion centers, numerous visits, and time commitment High Proptosis, High CAS TED Patients 5 – Burdensome reimbursement approval process 3 – Need for serial audiograms 1. Horizon Q3 2022
earnings call; LTM = last twelve months 4. Kahaly et al., Thyroid (2021) (ATA 2021 presentation) 17 2. Tourmaline market research 5. Horizon Q2 2023 10Q 3. TEPEZZA FDA label % of Patients
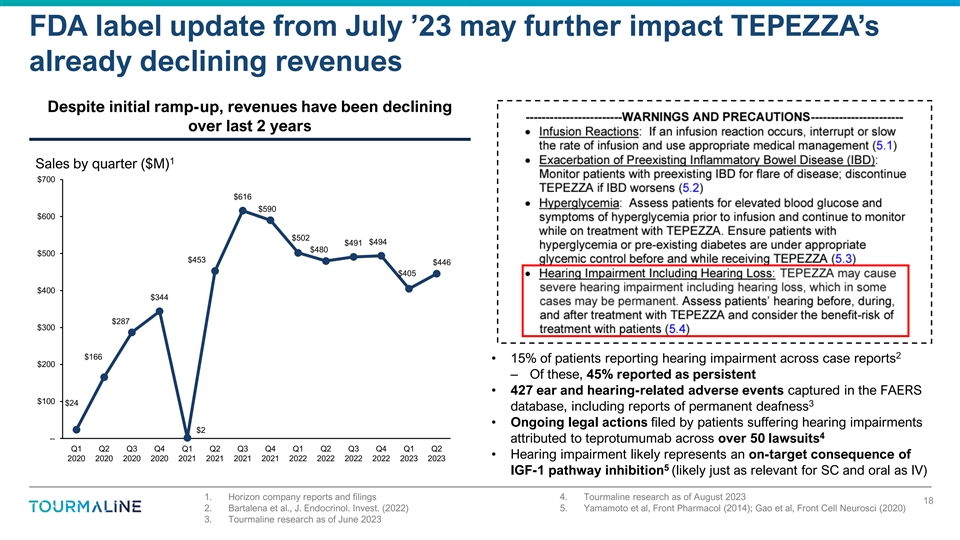
FDA label update from July ’23 may further impact TEPEZZA’s
already declining revenues Despite initial ramp-up, revenues have been declining over last 2 years 1 Sales by quarter ($M) $700 $616 $590 $600 $502 $494 $491 $480 $500 $453 $446 $405 $400 $344 $287 $300 2 $166 • 15% of patients reporting
hearing impairment across case reports $200 – Of these, 45% reported as persistent • 427 ear and hearing-related adverse events captured in the FAERS $100 $24 3 database, including reports of permanent deafness • Ongoing legal
actions filed by patients suffering hearing impairments $2 4 -- attributed to teprotumumab across over 50 lawsuits Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 • Hearing impairment likely represents an on-target consequence of 2020 2020 2020 2020
2021 2021 2021 2021 2022 2022 2022 2022 2023 2023 5 IGF-1 pathway inhibition (likely just as relevant for SC and oral as IV) 1. Horizon company reports and filings 4. Tourmaline research as of August 2023 18 2. Bartalena et al., J. Endocrinol.
Invest. (2022) 5. Yamamoto et al, Front Pharmacol (2014); Gao et al, Front Cell Neurosci (2020) 3. Tourmaline research as of June 2023
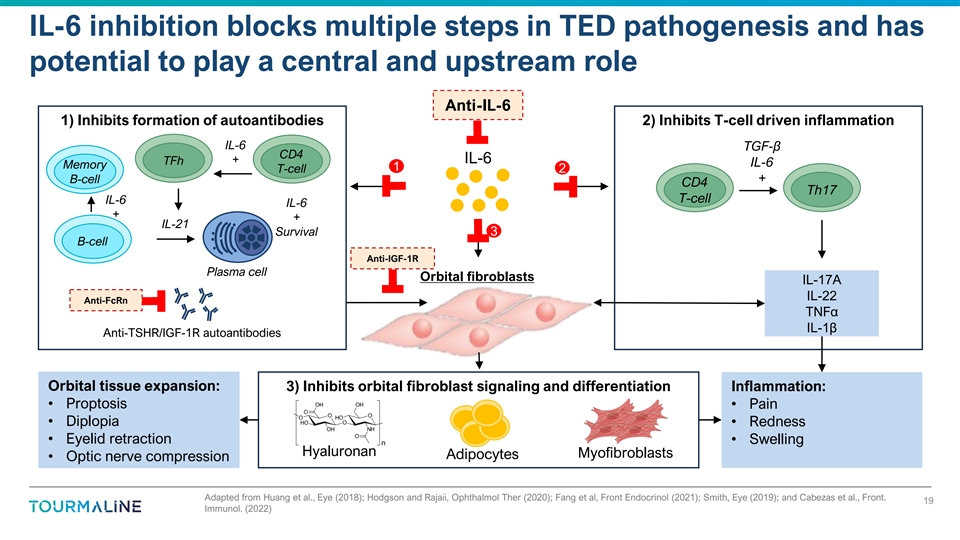
IL-6 inhibition blocks multiple steps in TED pathogenesis and has
potential to play a central and upstream role Anti-IL-6 1) Inhibits formation of autoantibodies 2) Inhibits T-cell driven inflammation IL-6 TGF-β CD4 + IL-6 TFh IL-6 Memory 1 T-cell 2 + B-cell CD4 Th17 T-cell IL-6 IL-6 + + IL-21 Survival 3
B-cell Anti-IGF-1R Plasma cell Orbital fibroblasts IL-17A IL-22 Anti-FcRn TNFα IL-1β Anti-TSHR/IGF-1R autoantibodies Orbital tissue expansion: 3) Inhibits orbital fibroblast signaling and differentiation Inflammation: • Proptosis
• Pain • Diplopia • Redness • Eyelid retraction • Swelling Hyaluronan Myofibroblasts Adipocytes • Optic nerve compression Adapted from Huang et al., Eye (2018); Hodgson and Rajaii, Ophthalmol Ther (2020); Fang et
al, Front Endocrinol (2021); Smith, Eye (2019); and Cabezas et al., Front. 19 Immunol. (2022)
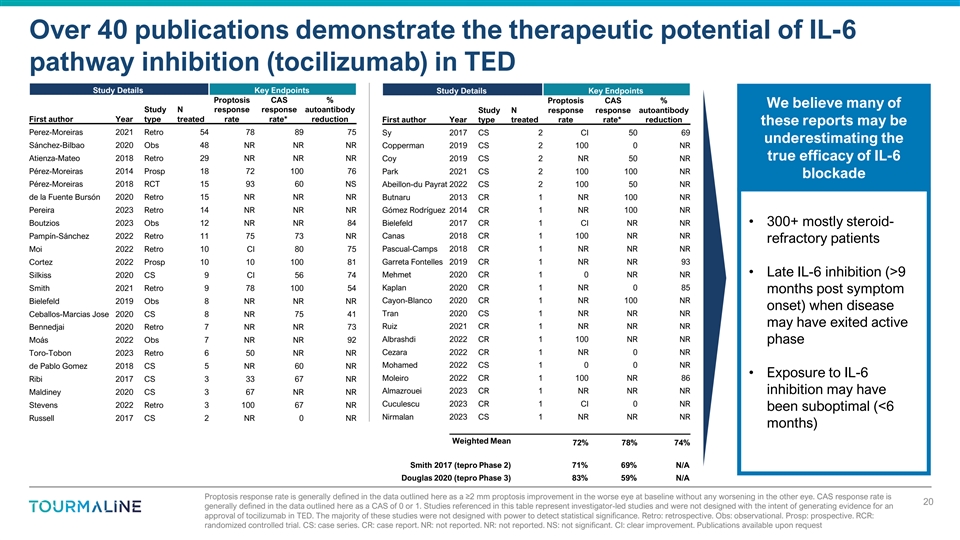
Over 40 publications demonstrate the therapeutic potential of IL-6
pathway inhibition (tocilizumab) in TED Study Details Key Endpoints Study Details Key Endpoints Proptosis CAS % Proptosis CAS % We believe many of Study N response response autoantibody Study N response response autoantibody First author Year type
treated rate rate* reduction First author Year type treated rate rate* reduction these reports may be Perez-Moreiras 2021 Retro 54 78 89 75 Sy 2017 CS 2 CI 50 69 underestimating the Sánchez-Bilbao 2020 Obs 48 NR NR NR Copperman 2019 CS 2 100 0
NR Atienza-Mateo 2018 Retro 29 NR NR NR Coy 2019 CS 2 NR 50 NR true efficacy of IL-6 Pérez-Moreiras 2014 Prosp 18 72 100 76 Park 2021 CS 2 100 100 NR blockade Pérez-Moreiras 2018 RCT 15 93 60 NS Abeillon-du Payrat 2022 CS 2 100 50 NR de la
Fuente Bursón 2020 Retro 15 NR NR NR Butnaru 2013 CR 1 NR 100 NR Pereira 2023 Retro 14 NR NR NR Gómez Rodríguez 2014 CR 1 NR 100 NR Boutzios 2023 Obs 12 NR NR 84 Bielefeld 2017 CR 1 CI NR NR • 300+ mostly steroid-
Pampín-Sánchez 2022 Retro 11 75 73 NR Canas 2018 CR 1 100 NR NR refractory patients Moi 2022 Retro 10 CI 80 75 Pascual-Camps 2018 CR 1 NR NR NR Cortez 2022 Prosp 10 10 100 81 Garreta Fontelles 2019 CR 1 NR NR 93 Mehmet 2020 CR 1 0 NR NR
• Late IL-6 inhibition (>9 Silkiss 2020 CS 9 CI 56 74 Smith 2021 Retro 9 78 100 54 Kaplan 2020 CR 1 NR 0 85 months post symptom Bielefeld 2019 Obs 8 NR NR NR Cayon-Blanco 2020 CR 1 NR 100 NR onset) when disease Tran 2020 CS 1 NR NR NR
Ceballos-Marcias Jose 2020 CS 8 NR 75 41 may have exited active Ruiz 2021 CR 1 NR NR NR Bennedjai 2020 Retro 7 NR NR 73 Moás 2022 Obs 7 NR NR 92 Albrashdi 2022 CR 1 100 NR NR phase Cezara 2022 CR 1 NR 0 NR Toro-Tobon 2023 Retro 6 50 NR NR
Mohamed 2022 CS 1 0 0 NR de Pablo Gomez 2018 CS 5 NR 60 NR • Exposure to IL-6 Moleiro 2022 CR 1 100 NR 86 Ribi 2017 CS 3 33 67 NR Almazrouei 2023 CR 1 NR NR NR Maldiney 2020 CS 3 67 NR NR inhibition may have Cuculescu 2023 CR 1 CI 0 NR Stevens
2022 Retro 3 100 67 NR been suboptimal (<6 Nirmalan 2023 CS 1 NR NR NR Russell 2017 CS 2 NR 0 NR months) Weighted Mean 72% 78% 74% Smith 2017 (tepro Phase 2) 71% 69% N/A Douglas 2020 (tepro Phase 3) 83% 59% N/A Proptosis response rate is
generally defined in the data outlined here as a ≥2 mm proptosis improvement in the worse eye at baseline without any worsening in the other eye. CAS response rate is 20 generally defined in the data outlined here as a CAS of 0 or 1. Studies
referenced in this table represent investigator-led studies and were not designed with the intent of generating evidence for an approval of tocilizumab in TED. The majority of these studies were not designed with power to detect statistical
significance. Retro: retrospective. Obs: observational. Prosp: prospective. RCR: randomized controlled trial. CS: case series. CR: case report. NR: not reported. NR: not reported. NS: not significant. CI: clear improvement. Publications available
upon request
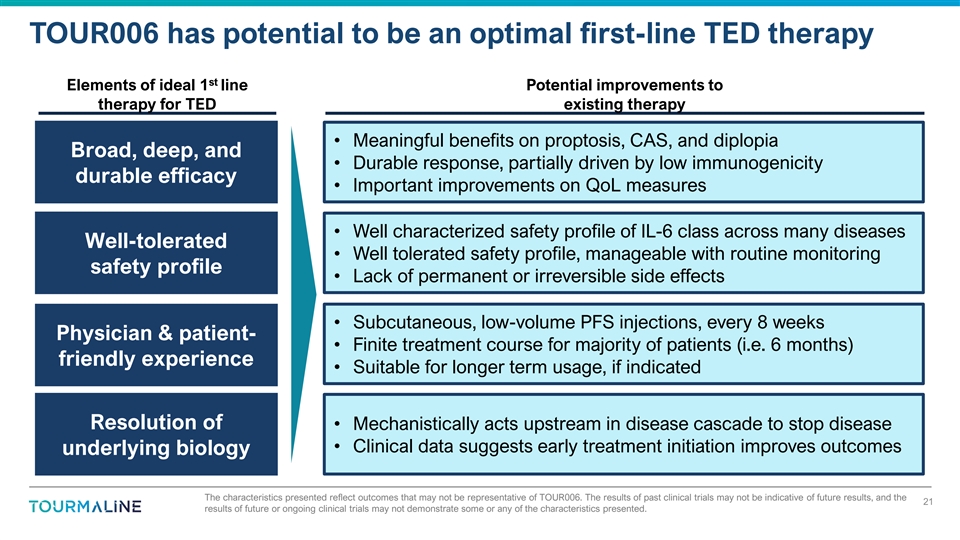
TOUR006 has potential to be an optimal first-line TED therapy st
Elements of ideal 1 line Potential improvements to therapy for TED existing therapy • Meaningful benefits on proptosis, CAS, and diplopia Broad, deep, and • Durable response, partially driven by low immunogenicity durable efficacy
• Important improvements on QoL measures • Well characterized safety profile of IL-6 class across many diseases Well-tolerated • Well tolerated safety profile, manageable with routine monitoring safety profile • Lack of
permanent or irreversible side effects • Subcutaneous, low-volume PFS injections, every 8 weeks Physician & patient- • Finite treatment course for majority of patients (i.e. 6 months) friendly experience • Suitable for longer
term usage, if indicated Resolution of • Mechanistically acts upstream in disease cascade to stop disease • Clinical data suggests early treatment initiation improves outcomes underlying biology The characteristics presented reflect
outcomes that may not be representative of TOUR006. The results of past clinical trials may not be indicative of future results, and the 21 results of future or ongoing clinical trials may not demonstrate some or any of the characteristics
presented.
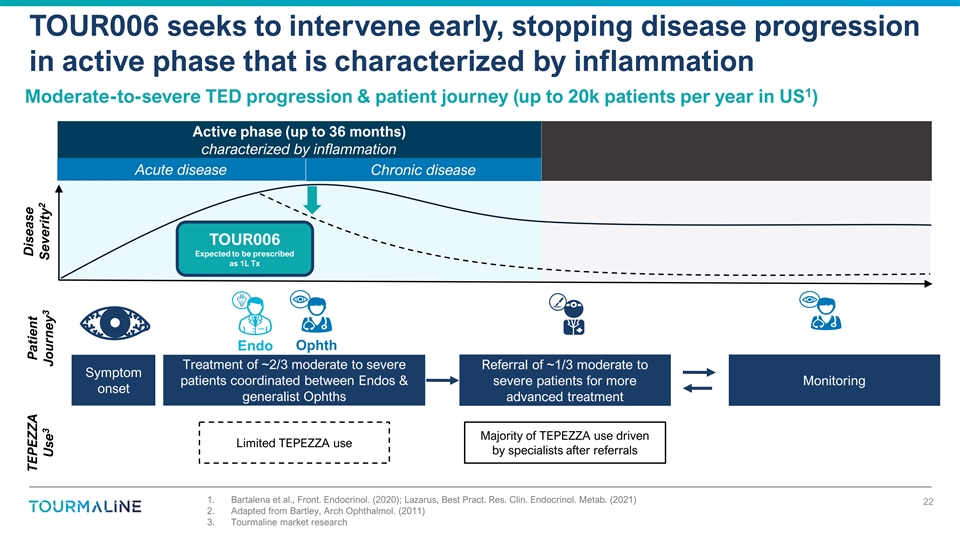
TOUR006 seeks to intervene early, stopping disease progression in
active phase that is characterized by inflammation 1 Moderate-to-severe TED progression & patient journey (up to 20k patients per year in US ) Active phase (up to 36 months) characterized by inflammation Acute disease Chronic disease TOUR006
Expected to be prescribed as 1L Tx Endo Ophth Treatment of ~2/3 moderate to severe Referral of ~1/3 moderate to Symptom patients coordinated between Endos & severe patients for more Monitoring onset generalist Ophths advanced treatment Majority
of TEPEZZA use driven Limited TEPEZZA use by specialists after referrals 1. Bartalena et al., Front. Endocrinol. (2020); Lazarus, Best Pract. Res. Clin. Endocrinol. Metab. (2021) 22 2. Adapted from Bartley, Arch Ophthalmol. (2011) 3. Tourmaline
market research Disease TEPEZZA Patient 2 3 3 Severity Use Journey
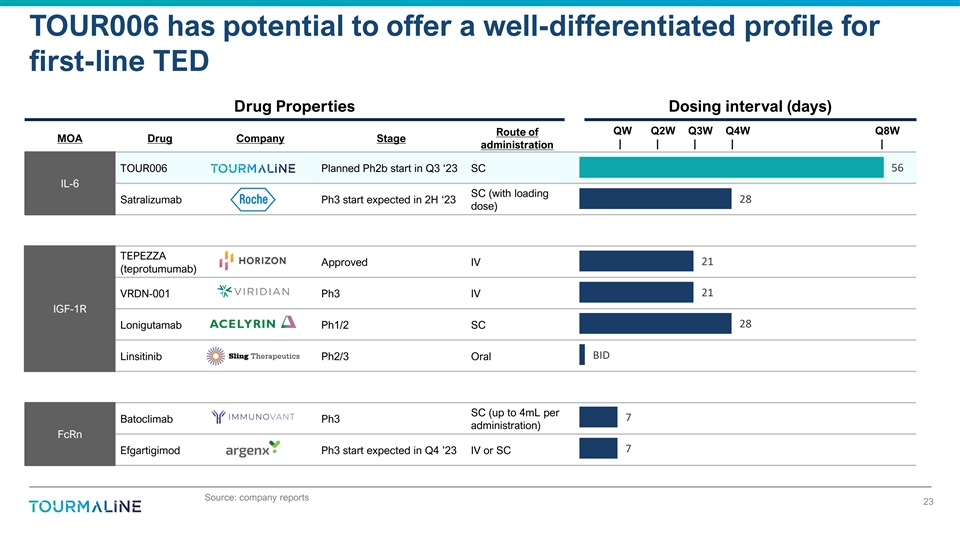
TOUR006 has potential to offer a well-differentiated profile for
first-line TED Drug Properties Dosing interval (days) QW Q2W Q3W Q4W Q8W Route of MOA Drug Company Stage | | | | | administration TOUR006 Planned Ph2b start in Q3 ‘23 SC 56 IL-6 SC (with loading 28 Satralizumab Ph3 start expected in 2H
‘23 dose) TEPEZZA 21 Approved IV (teprotumumab) 21 VRDN-001 Ph3 IV IGF-1R 28 Lonigutamab Ph1/2 SC BID Linsitinib Ph2/3 Oral SC (up to 4mL per 7 Batoclimab Ph3 administration) FcRn 7 Efgartigimod Ph3 start expected in Q4 ’23 IV or SC
Source: company reports 23
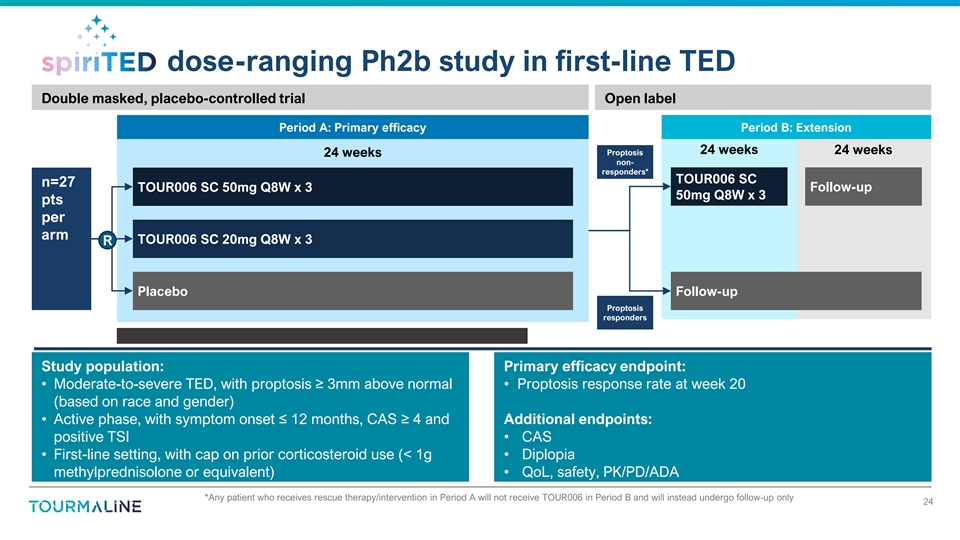
dose-ranging Ph2b study in first-line TED Double masked,
placebo-controlled trial Open label Period A: Primary efficacy Period B: Extension 24 weeks 24 weeks Proptosis 24 weeks non- responders* TOUR006 SC n=27 TOUR006 SC 50mg Q8W x 3 Follow-up 50mg Q8W x 3 pts per arm TOUR006 SC 20mg Q8W x 3 R Placebo
Follow-up Proptosis responders Study population: Primary efficacy endpoint: • Moderate-to-severe TED, with proptosis ≥ 3mm above normal • Proptosis response rate at week 20 (based on race and gender) • Active phase, with
symptom onset ≤ 12 months, CAS ≥ 4 and Additional endpoints: positive TSI • CAS • First-line setting, with cap on prior corticosteroid use (< 1g • Diplopia methylprednisolone or equivalent) • QoL, safety,
PK/PD/ADA *Any patient who receives rescue therapy/intervention in Period A will not receive TOUR006 in Period B and will instead undergo follow-up only 24
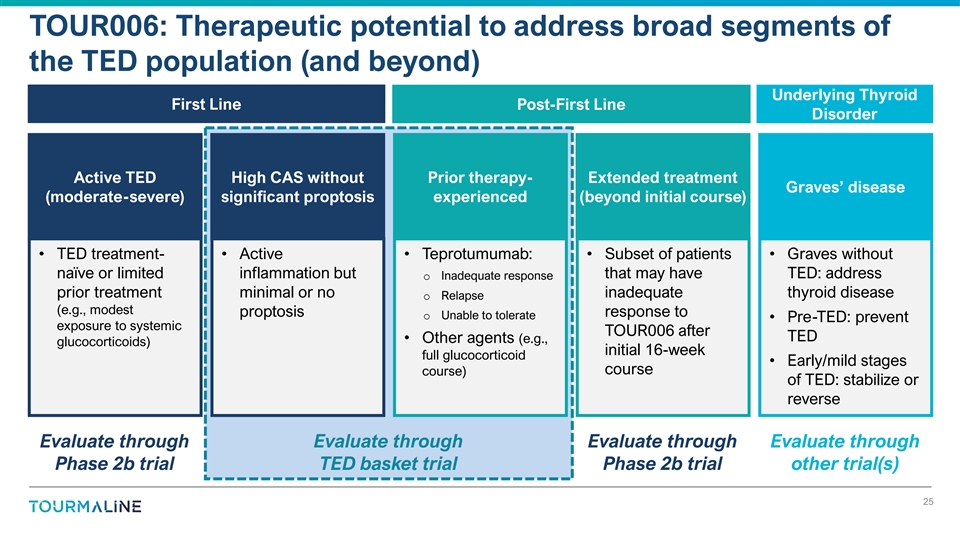
TOUR006: Therapeutic potential to address broad segments of the TED
population (and beyond) Underlying Thyroid First Line Post-First Line Disorder Active TED High CAS without Prior therapy- Extended treatment Graves’ disease (moderate-severe) significant proptosis experienced (beyond initial course) •
TED treatment- • Active • Teprotumumab: • Subset of patients • Graves without naïve or limited inflammation but that may have TED: address o Inadequate response prior treatment minimal or no inadequate thyroid disease o
Relapse (e.g., modest proptosis response to o Unable to tolerate • Pre-TED: prevent exposure to systemic TOUR006 after TED • Other agents (e.g., glucocorticoids) initial 16-week full glucocorticoid • Early/mild stages course
course) of TED: stabilize or reverse Evaluate through Evaluate through Evaluate through Evaluate through Phase 2b trial TED basket trial Phase 2b trial other trial(s) 25
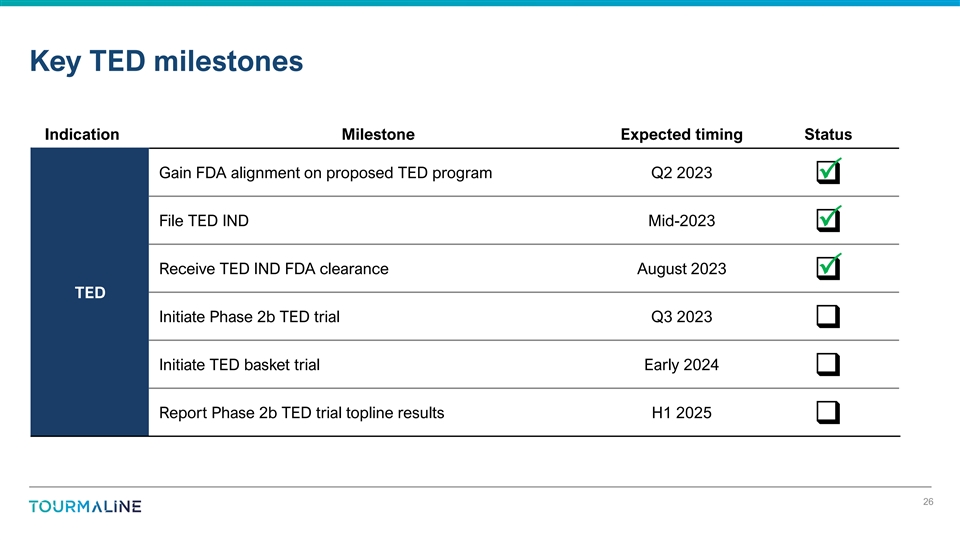
Key TED milestones Indication Milestone Expected timing Status Gain FDA
alignment on proposed TED program Q2 2023 P q File TED IND Mid-2023 P q Receive TED IND FDA clearance August 2023 P q TED Initiate Phase 2b TED trial Q3 2023 q Initiate TED basket trial Early 2024 q Report Phase
2b TED trial topline results H1 2025 q 26
Atherosclerotic Cardiovascular Disease (ASCVD)
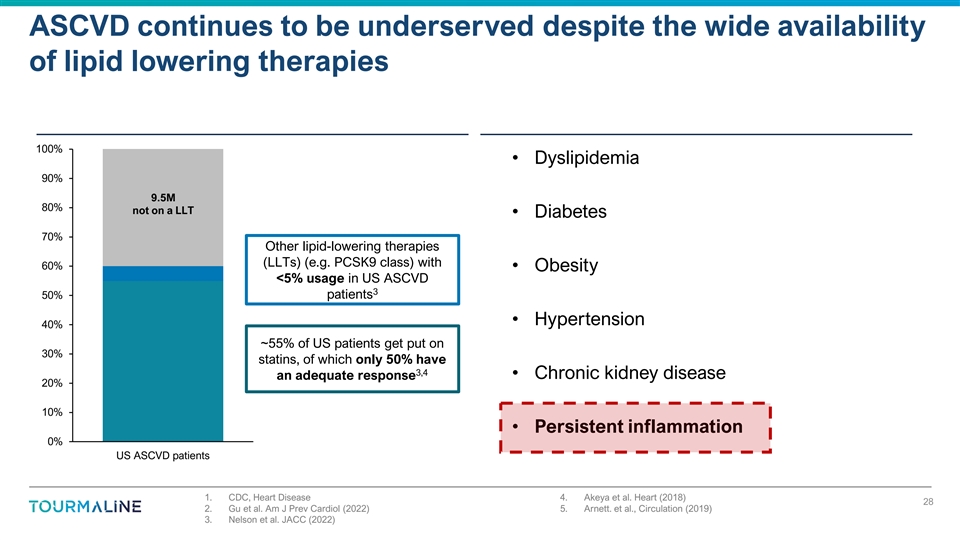
ASCVD continues to be underserved despite the wide availability of
lipid lowering therapies 100% • Dyslipidemia 90% 9.5M 80% not on a LLT • Diabetes 70% Other lipid-lowering therapies (LLTs) (e.g. PCSK9 class) with 60% • Obesity <5% usage in US ASCVD 3 50% patients • Hypertension 40% ~55%
of US patients get put on 30% statins, of which only 50% have 3,4 • Chronic kidney disease an adequate response 20% 10% • Persistent inflammation 0% US ASCVD patients 1. CDC, Heart Disease 4. Akeya et al. Heart (2018) 28 2. Gu et al. Am
J Prev Cardiol (2022) 5. Arnett. et al., Circulation (2019) 3. Nelson et al. JACC (2022)
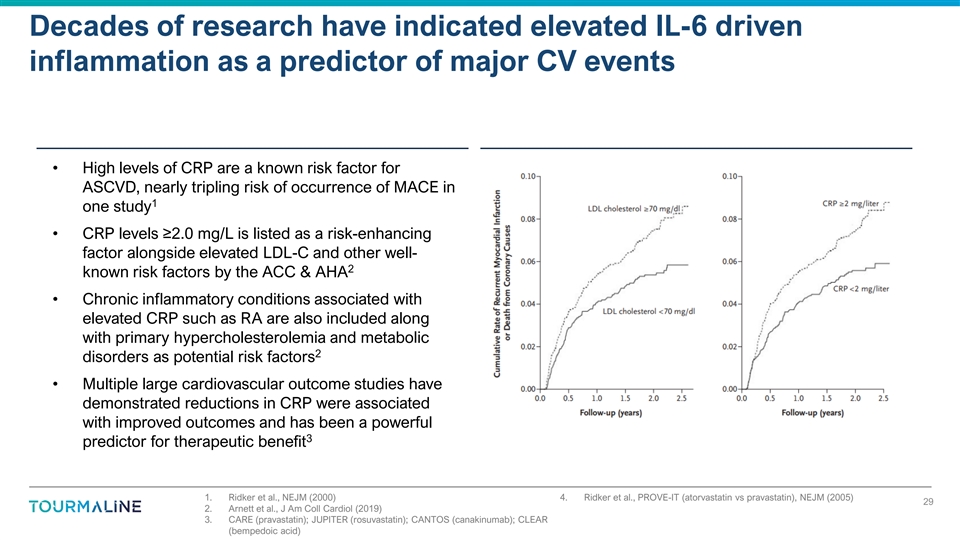
Decades of research have indicated elevated IL-6 driven inflammation as
a predictor of major CV events • High levels of CRP are a known risk factor for ASCVD, nearly tripling risk of occurrence of MACE in 1 one study • CRP levels ≥2.0 mg/L is listed as a risk-enhancing factor alongside elevated LDL-C
and other well- 2 known risk factors by the ACC & AHA • Chronic inflammatory conditions associated with elevated CRP such as RA are also included along with primary hypercholesterolemia and metabolic 2 disorders as potential risk factors
• Multiple large cardiovascular outcome studies have demonstrated reductions in CRP were associated with improved outcomes and has been a powerful 3 predictor for therapeutic benefit 1. Ridker et al., NEJM (2000) 4. Ridker et al., PROVE-IT
(atorvastatin vs pravastatin), NEJM (2005) 29 2. Arnett et al., J Am Coll Cardiol (2019) 3. CARE (pravastatin); JUPITER (rosuvastatin); CANTOS (canakinumab); CLEAR (bempedoic acid)
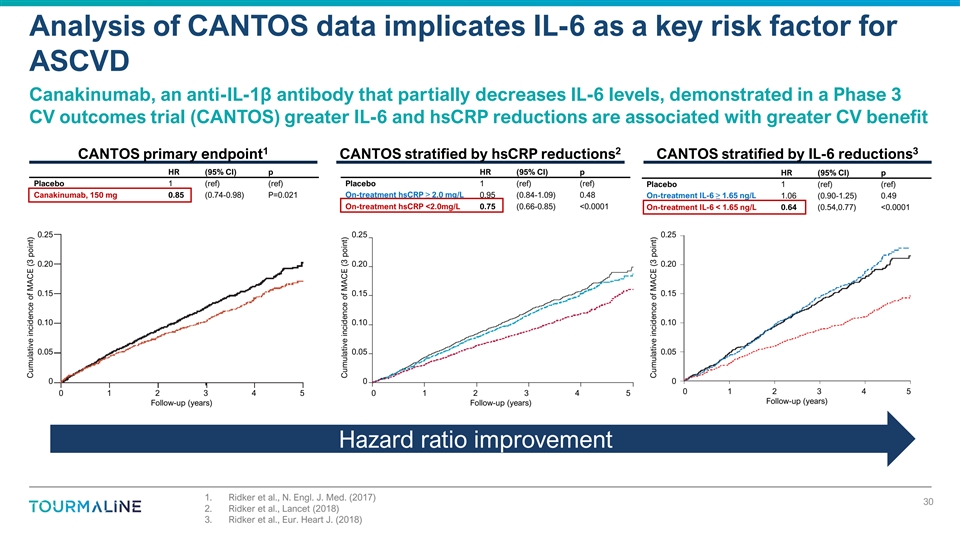
Analysis of CANTOS data implicates IL-6 as a key risk factor for ASCVD
Canakinumab, an anti-IL-1β antibody that partially decreases IL-6 levels, demonstrated in a Phase 3 CV outcomes trial (CANTOS) greater IL-6 and hsCRP reductions are associated with greater CV benefit 1 2 3 CANTOS primary endpoint CANTOS
stratified by hsCRP reductions CANTOS stratified by IL-6 reductions HR (95% CI) p HR (95% CI) p HR (95% CI) p Placebo 1 (ref) (ref) Placebo 1 (ref) (ref) Placebo 1 (ref) (ref) On-treatment hsCRP≥ 2.0 mg/L Canakinumab, 150 mg 0.85 (0.74-0.98)
P=0.021 0.95 (0.84-1.09) 0.48 On-treatment IL-6 ≥ 1.65 ng/L 1.06 (0.90-1.25) 0.49 On-treatment hsCRP <2.0mg/L 0.75 (0.66-0.85) <0.0001 On-treatment IL-6 < 1.65 ng/L 0.64 (0.54,0.77) <0.0001 0.25 0.25 0.25 0.20 0.20 0.20 0.15 0.15
0.15 0.10 0.10 0.10 0.05 0.05 0.05 0 0 0 0 1 2 3 4 5 0 1 2 3 4 5 0 1 2 3 4 5 Follow-up (years) Follow-up (years) Follow-up (years) Hazard ratio improvement 1. Ridker et al., N. Engl. J. Med. (2017) 30 2. Ridker et al., Lancet (2018) 3. Ridker et
al., Eur. Heart J. (2018) Cumulative incidence of MACE (3 point) Cumulative incidence of MACE (3 point) Cumulative incidence of MACE (3 point)
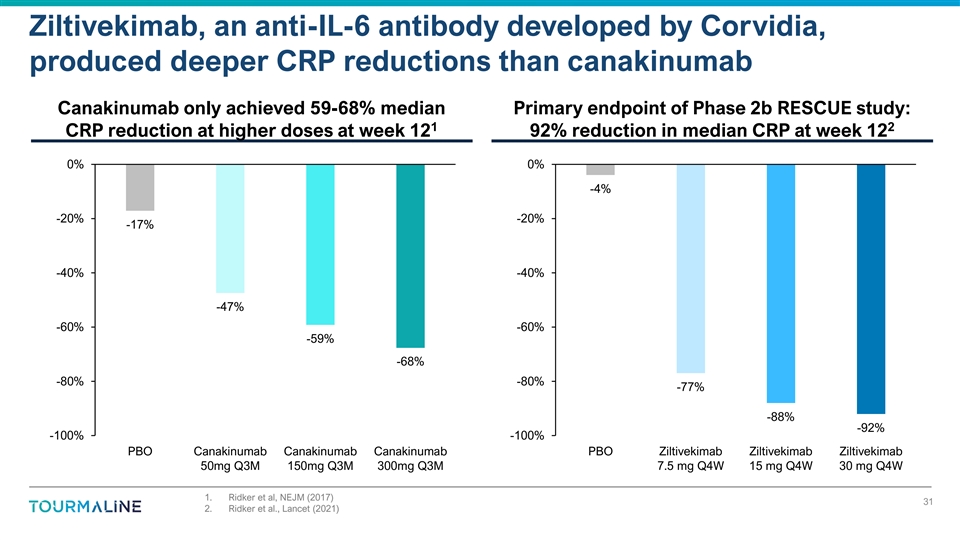
Ziltivekimab, an anti-IL-6 antibody developed by Corvidia, produced
deeper CRP reductions than canakinumab Canakinumab only achieved 59-68% median Primary endpoint of Phase 2b RESCUE study: 1 2 CRP reduction at higher doses at week 12 92% reduction in median CRP at week 12 0% 0% -4% -20% -20% -17% -40% -40% -47%
-60% -60% -59% -68% -80% -80% -77% -88% -92% -100% -100% PBO Canakinumab Canakinumab Canakinumab PBO Ziltivekimab Ziltivekimab Ziltivekimab 50mg Q3M 150mg Q3M 300mg Q3M 7.5 mg Q4W 15 mg Q4W 30 mg Q4W 1. Ridker et al, NEJM (2017) 31 2. Ridker et al.,
Lancet (2021)
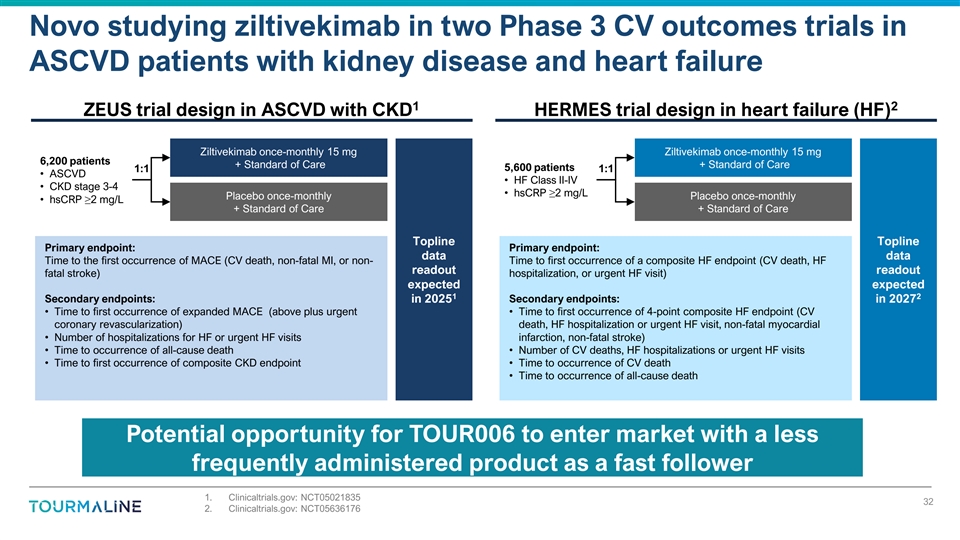
Novo studying ziltivekimab in two Phase 3 CV outcomes trials in ASCVD
patients with kidney disease and heart failure 1 2 ZEUS trial design in ASCVD with CKD HERMES trial design in heart failure (HF) Ziltivekimab once-monthly 15 mg Ziltivekimab once-monthly 15 mg 6,200 patients + Standard of Care + Standard of Care
5,600 patients 1:1 1:1 • ASCVD • HF Class II-IV • CKD stage 3-4 • hsCRP≥2 mg/L Placebo once-monthly Placebo once-monthly • hsCRP≥2 mg/L + Standard of Care + Standard of Care Topline Topline Primary endpoint:
Primary endpoint: data data Time to the first occurrence of MACE (CV death, non-fatal MI, or non- Time to first occurrence of a composite HF endpoint (CV death, HF readout readout fatal stroke) hospitalization, or urgent HF visit) expected expected
1 2 Secondary endpoints: in 2025 Secondary endpoints: in 2027 • Time to first occurrence of expanded MACE (above plus urgent • Time to first occurrence of 4-point composite HF endpoint (CV coronary revascularization) death, HF
hospitalization or urgent HF visit, non-fatal myocardial • Number of hospitalizations for HF or urgent HF visits infarction, non-fatal stroke) • Time to occurrence of all-cause death • Number of CV deaths, HF hospitalizations or
urgent HF visits • Time to first occurrence of composite CKD endpoint • Time to occurrence of CV death • Time to occurrence of all-cause death Potential opportunity for TOUR006 to enter market with a less frequently administered
product as a fast follower 1. Clinicaltrials.gov: NCT05021835 32 2. Clinicaltrials.gov: NCT05636176
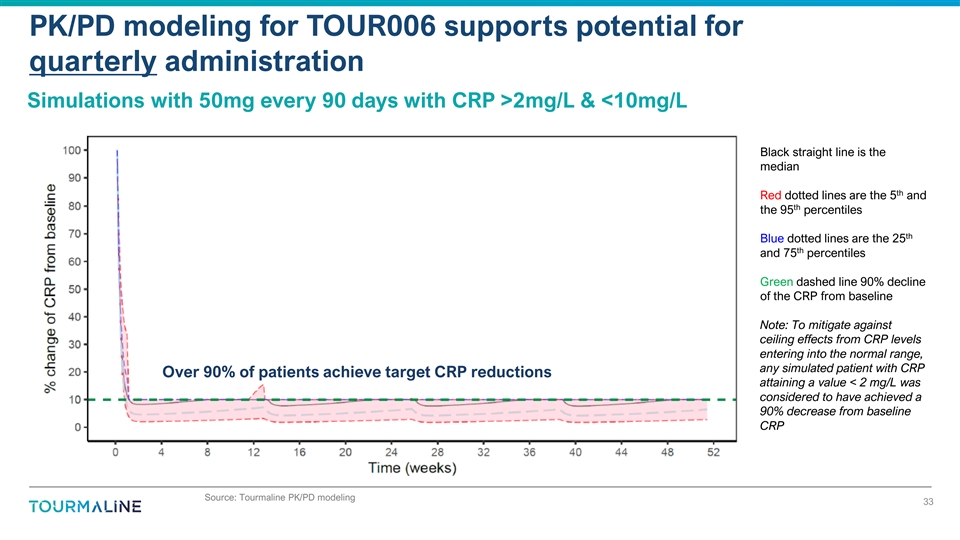
PK/PD modeling for TOUR006 supports potential for quarterly
administration Simulations with 50mg every 90 days with CRP >2mg/L & <10mg/L Black straight line is the median th Red dotted lines are the 5 and th the 95 percentiles th Blue dotted lines are the 25 th and 75 percentiles Green dashed line
90% decline of the CRP from baseline Note: To mitigate against ceiling effects from CRP levels entering into the normal range, any simulated patient with CRP Over 90% of patients achieve target CRP reductions attaining a value < 2 mg/L was
considered to have achieved a 90% decrease from baseline CRP Source: Tourmaline PK/PD modeling 33
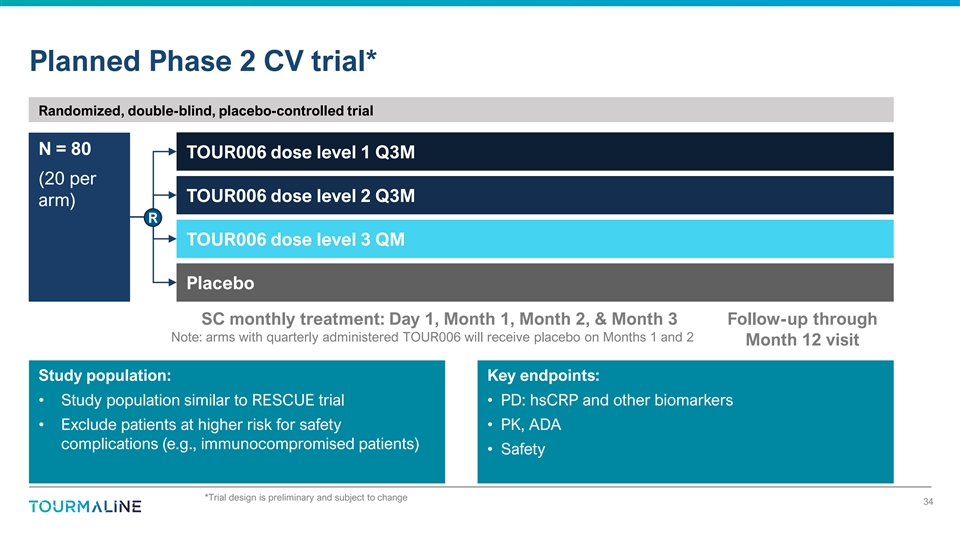
Planned Phase 2 CV trial* Randomized, double-blind, placebo-controlled
trial N = 80 TOUR006 dose level 1 Q3M (20 per TOUR006 dose level 2 Q3M arm) R TOUR006 dose level 3 QM Placebo SC monthly treatment: Day 1, Month 1, Month 2, & Month 3 Follow-up through Note: arms with quarterly administered TOUR006 will receive
placebo on Months 1 and 2 Month 12 visit Study population: Key endpoints: • Study population similar to RESCUE trial • PD: hsCRP and other biomarkers • Exclude patients at higher risk for safety • PK, ADA complications (e.g.,
immunocompromised patients) • Safety *Trial design is preliminary and subject to change 34
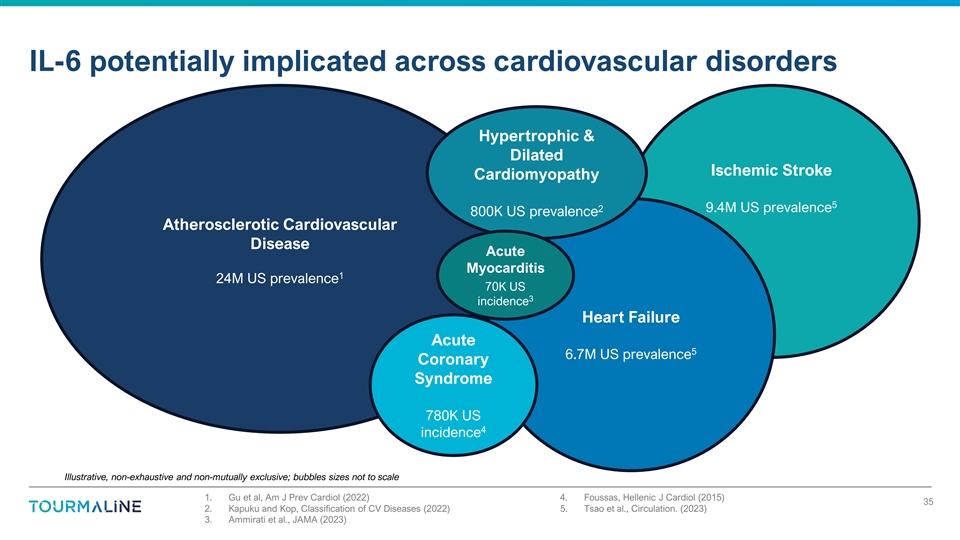
IL-6 potentially implicated across cardiovascular disorders
Hypertrophic & Dilated Ischemic Stroke Cardiomyopathy 5 2 9.4M US prevalence 800K US prevalence Atherosclerotic Cardiovascular Disease Acute Myocarditis 1 24M US prevalence 70K US 3 incidence Heart Failure Acute 5 6.7M US prevalence Coronary
Syndrome 780K US 4 incidence Illustrative, non-exhaustive and non-mutually exclusive; bubbles sizes not to scale 1. Gu et al, Am J Prev Cardiol (2022) 4. Foussas, Hellenic J Cardiol (2015) 35 2. Kapuku and Kop, Classification of CV Diseases (2022)
5. Tsao et al., Circulation. (2023) 3. Ammirati et al., JAMA (2023)
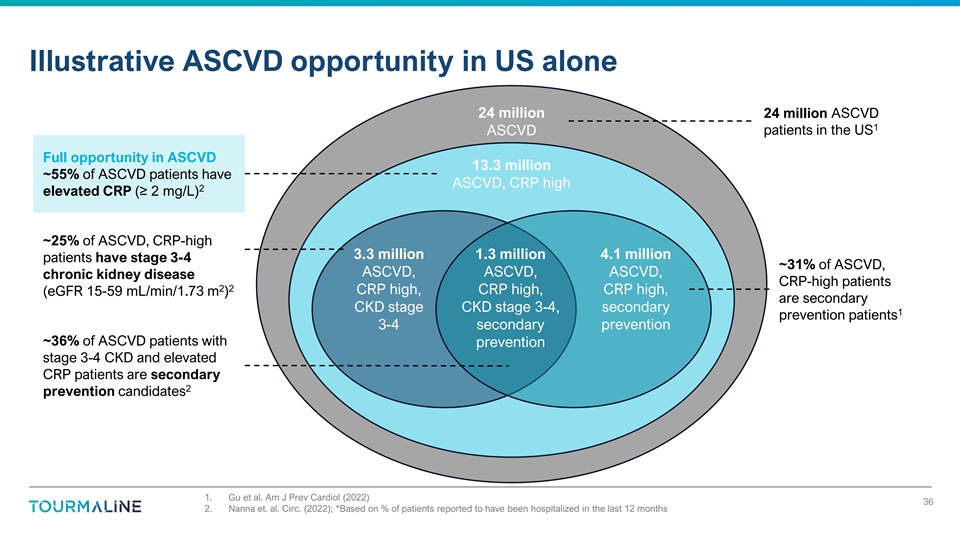
Illustrative ASCVD opportunity in US alone 24 million 24 million ASCVD
1 patients in the US ASCVD Full opportunity in ASCVD 13.3 million ~55% of ASCVD patients have ASCVD, CRP high 2 elevated CRP (≥ 2 mg/L) ~25% of ASCVD, CRP-high 3.3 million 1.3 million 4.1 million patients have stage 3-4 ~31% of ASCVD, ASCVD,
ASCVD, ASCVD, chronic kidney disease CRP-high patients 2 2 CRP high, CRP high, CRP high, (eGFR 15-59 mL/min/1.73 m ) are secondary CKD stage CKD stage 3-4, secondary 1 prevention patients 3-4 secondary prevention ~36% of ASCVD patients with
prevention stage 3-4 CKD and elevated CRP patients are secondary 2 prevention candidates 1. Gu et al. Am J Prev Cardiol (2022) 36 2. Nanna et. al. Circ. (2022); *Based on % of patients reported to have been hospitalized in the last 12
months
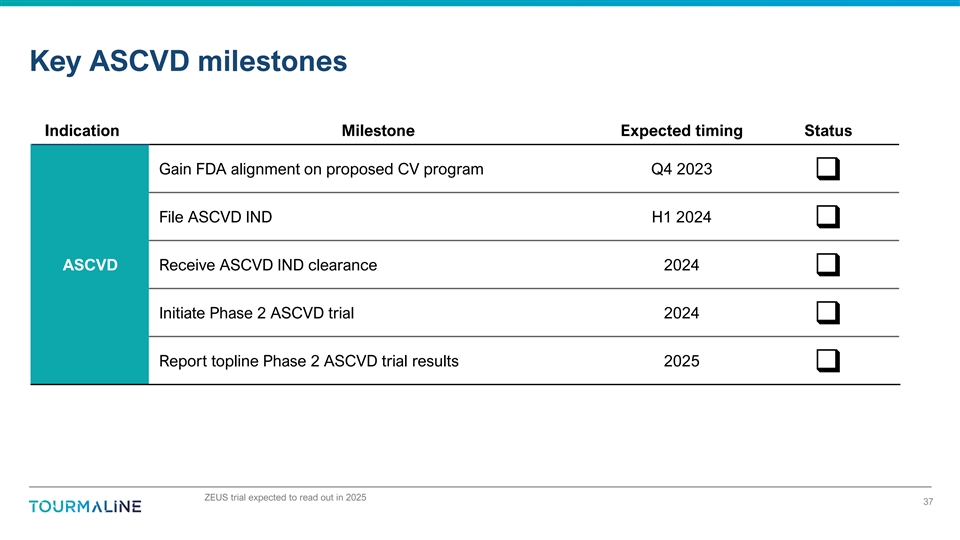
Key ASCVD milestones Indication Milestone Expected timing Status Gain
FDA alignment on proposed CV program Q4 2023 q File ASCVD IND H1 2024 q ASCVD Receive ASCVD IND clearance 2024 q Initiate Phase 2 ASCVD trial 2024 q Report topline Phase 2 ASCVD trial results 2025 q ZEUS trial expected to
read out in 2025 37

Key Business Items
Terms of TOUR006 license with Pfizer In May 2022, Tourmaline obtained
an exclusive global license to TOUR006 (formerly PF-04236921) from Pfizer in exchange for: § $5M upfront payment and 15% equity of Tourmaline § Milestones: o Up to $128M in development and regulatory milestones o Up to $525M in sales-based
milestones § Low double-digit (less than 15%) royalties on net sales, subject to specified royalty reductions § Additional payments due upon out-license/divestiture of TOUR006 in major market § Right of first negotiation for Pfizer
should Tourmaline seek to out-license or partner in the US 40
TOUR006 regulatory exclusivity and intellectual property Regulatory
Exclusivity • In the US, we expect to rely on 12 years’ data exclusivity for biologics • Regulatory counsel has confirmed this is a reasonable expectation Patent Protection • We have filed 5 new patent applications on TOUR006
• Incorporating claims on: • Indication-specific methods of use • Dosing regimens • If issued, will expire in 2043 (or later) • Additional patent applications in process • Pfizer has abandoned all previous Pfizer
patents/applications relating to TOUR006 • No freedom to operate issues identified 41
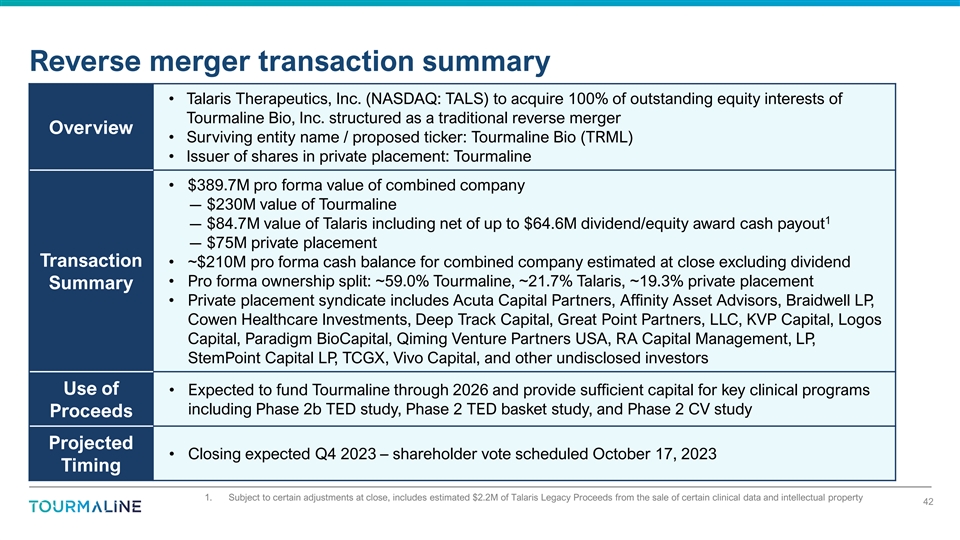
Reverse merger transaction summary • Talaris Therapeutics, Inc.
(NASDAQ: TALS) to acquire 100% of outstanding equity interests of Tourmaline Bio, Inc. structured as a traditional reverse merger Overview • Surviving entity name / proposed ticker: Tourmaline Bio (TRML) • Issuer of shares in private
placement: Tourmaline • $389.7M pro forma value of combined company ― $230M value of Tourmaline 1 ― $84.7M value of Talaris including net of up to $64.6M dividend/equity award cash payout ― $75M private placement Transaction
• ~$210M pro forma cash balance for combined company estimated at close excluding dividend • Pro forma ownership split: ~59.0% Tourmaline, ~21.7% Talaris, ~19.3% private placement Summary • Private placement syndicate includes
Acuta Capital Partners, Affinity Asset Advisors, Braidwell LP, Cowen Healthcare Investments, Deep Track Capital, Great Point Partners, LLC, KVP Capital, Logos Capital, Paradigm BioCapital, Qiming Venture Partners USA, RA Capital Management, LP,
StemPoint Capital LP, TCGX, Vivo Capital, and other undisclosed investors Use of • Expected to fund Tourmaline through 2026 and provide sufficient capital for key clinical programs including Phase 2b TED study, Phase 2 TED basket study, and
Phase 2 CV study Proceeds Projected • Closing expected Q4 2023 – shareholder vote scheduled October 17, 2023 Timing 1. Subject to certain adjustments at close, includes estimated $2.2M of Talaris Legacy Proceeds from the sale of certain
clinical data and intellectual property 42
Key highlights An IL-6 renaissance is underway: new insights emerging
about a broad range of indications where IL-6 may be clinically validated TOUR006 offers potential for low volume, infrequent subcutaneous administration We are rapidly advancing TOUR006 into mid/late-stage development Our team has extensive
experience developing and commercializing antibodies for orphan and autoimmune diseases Cash runway expected to fund development through 2026* *Upon completion of the merger with Talaris and pre-closing financing 43

Appendix
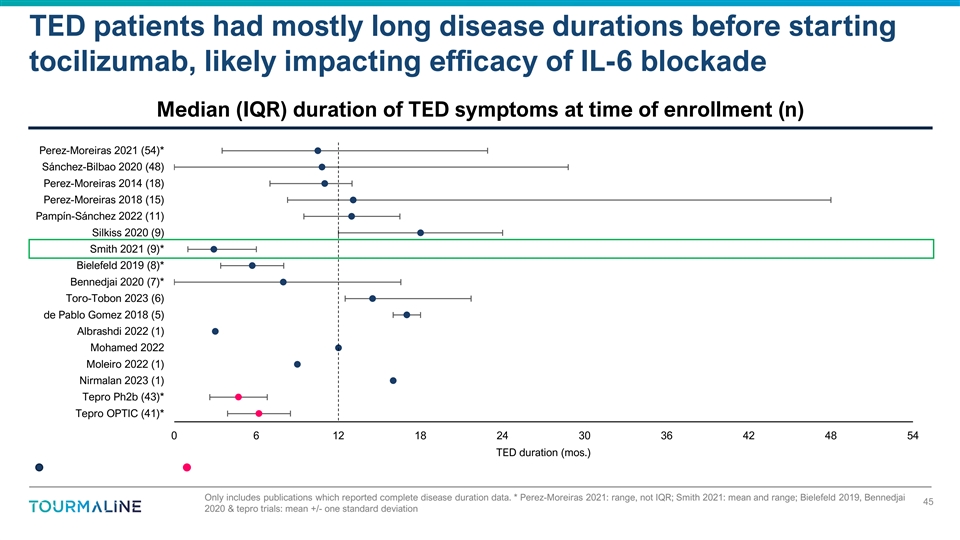
TED patients had mostly long disease durations before starting
tocilizumab, likely impacting efficacy of IL-6 blockade Median (IQR) duration of TED symptoms at time of enrollment (n) Perez-Moreiras 2021 (54)* Sánchez-Bilbao 2020 (48) Perez-Moreiras 2014 (18) Perez-Moreiras 2018 (15)
Pampín-Sánchez 2022 (11) Silkiss 2020 (9) Smith 2021 (9)* Bielefeld 2019 (8)* Bennedjai 2020 (7)* Toro-Tobon 2023 (6) de Pablo Gomez 2018 (5) Albrashdi 2022 (1) Mohamed 2022 Moleiro 2022 (1) Nirmalan 2023 (1) Tepro Ph2b (43)* Tepro OPTIC
(41)* 0 6 12 18 24 30 36 42 48 54 TED duration (mos.) Only includes publications which reported complete disease duration data. * Perez-Moreiras 2021: range, not IQR; Smith 2021: mean and range; Bielefeld 2019, Bennedjai 45 2020 & tepro trials:
mean +/- one standard deviation
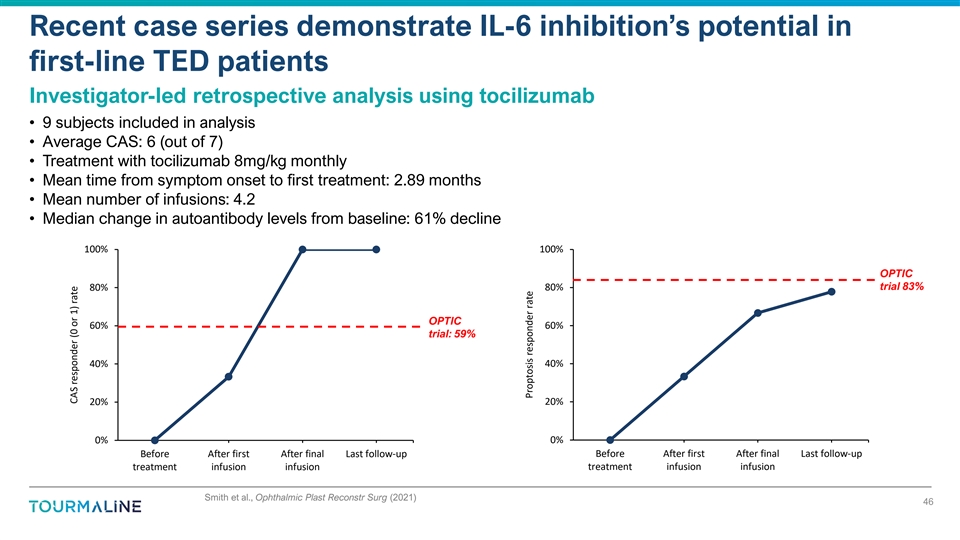
Recent case series demonstrate IL-6 inhibition’s potential in
first-line TED patients Investigator-led retrospective analysis using tocilizumab • 9 subjects included in analysis • Average CAS: 6 (out of 7) • Treatment with tocilizumab 8mg/kg monthly • Mean time from symptom onset to
first treatment: 2.89 months • Mean number of infusions: 4.2 • Median change in autoantibody levels from baseline: 61% decline 100% 100% OPTIC 80% 80% trial 83% OPTIC 60% 60% trial: 59% 40% 40% 20% 20% 0% 0% Before After first After
final Last follow-up Before After first After final Last follow-up treatment infusion infusion treatment infusion infusion Smith et al., Ophthalmic Plast Reconstr Surg (2021) 46 CAS responder (0 or 1) rate Proptosis responder rate
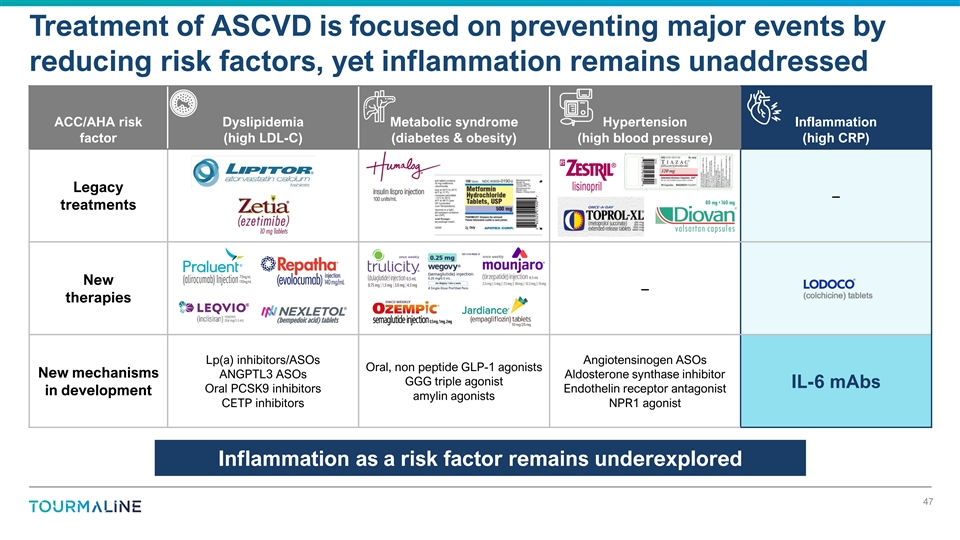
Treatment of ASCVD is focused on preventing major events by reducing
risk factors, yet inflammation remains unaddressed ACC/AHA risk Dyslipidemia Metabolic syndrome Hypertension Inflammation factor (high LDL-C) (diabetes & obesity) (high blood pressure) (high CRP) Legacy – treatments New – therapies
Lp(a) inhibitors/ASOs Angiotensinogen ASOs Oral, non peptide GLP-1 agonists New mechanisms ANGPTL3 ASOs Aldosterone synthase inhibitor GGG triple agonist IL-6 mAbs Oral PCSK9 inhibitors Endothelin receptor antagonist in development amylin agonists
CETP inhibitors NPR1 agonist Inflammation as a risk factor remains underexplored 47
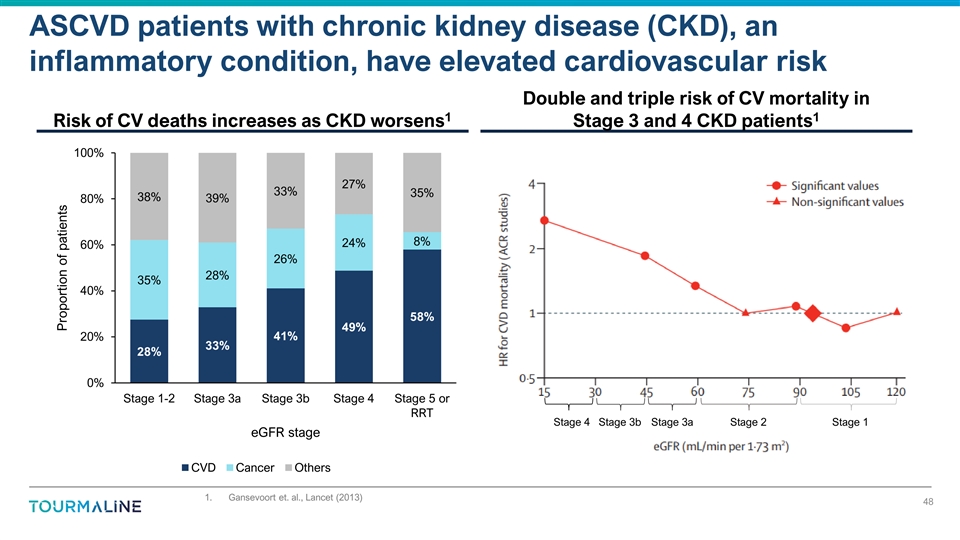
ASCVD patients with chronic kidney disease (CKD), an inflammatory
condition, have elevated cardiovascular risk Double and triple risk of CV mortality in 1 1 Risk of CV deaths increases as CKD worsens Stage 3 and 4 CKD patients 100% 27% 33% 35% 38% 80% 39% 8% 24% 60% 26% 28% 35% 40% 58% 49% 41% 20% 33% 28% 0% Stage
1-2 Stage 3a Stage 3b Stage 4 Stage 5 or RRT Stage 4 Stage 3b Stage 3a Stage 2 Stage 1 eGFR stage CVD Cancer Others 1. Gansevoort et. al., Lancet (2013) 48 Proportion of patients
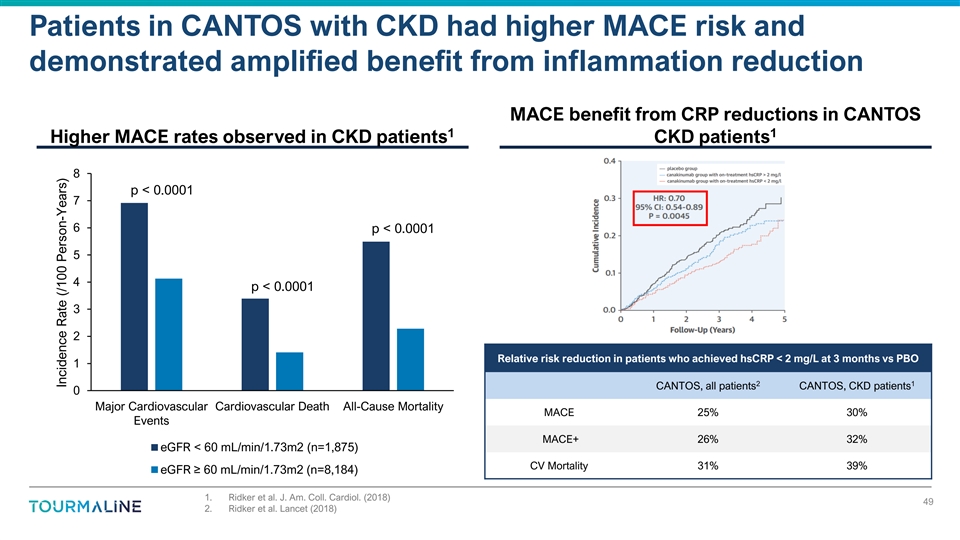
Patients in CANTOS with CKD had higher MACE risk and demonstrated
amplified benefit from inflammation reduction MACE benefit from CRP reductions in CANTOS 1 1 Higher MACE rates observed in CKD patients CKD patients 8 p < 0.0001 7 6 p < 0.0001 5 4 p < 0.0001 3 2 Relative risk reduction in patients who
achieved hsCRP < 2 mg/L at 3 months vs PBO 1 2 1 CANTOS, all patients CANTOS, CKD patients 0 Major Cardiovascular Cardiovascular Death All-Cause Mortality MACE 25% 30% Events MACE+ 26% 32% eGFR < 60 mL/min/1.73m2 (n=1,875) CV Mortality 31% 39%
eGFR ≥ 60 mL/min/1.73m2 (n=8,184) 1. Ridker et al. J. Am. Coll. Cardiol. (2018) 49 2. Ridker et al. Lancet (2018) Incidence Rate (/100 Person-Years)

Talaris Therapeutics (NASDAQ:TALS)
Historical Stock Chart
From Apr 2024 to May 2024

Talaris Therapeutics (NASDAQ:TALS)
Historical Stock Chart
From May 2023 to May 2024
