Savara Inc false 0001160308 0001160308 2024-01-05 2024-01-05
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, DC 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of The Securities Exchange Act of 1934
Date of Report (Date of earliest event reported)
January 5, 2024
SAVARA INC.
(Exact name of registrant as specified in its charter)
|
|
|
|
|
| Delaware |
|
001-32157 |
|
84-1318182 |
| (State or other jurisdiction of incorporation) |
|
(Commission File Number) |
|
(IRS Employer Identification No.) |
|
| 1717 Langhorne Newtown Road, Suite 300 |
| Langhorne, PA 19047 |
| (Address of principal executive offices, including zip code) |
(512) 614-1848
(Registrant’s telephone number, including area code)
N/A
(Former name or former address, if changed since last report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions (see General Instruction A.2. below):
| ☐ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ☐ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ☐ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ☐ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
|
|
|
|
|
| Title of each class |
|
Trading Symbol(s) |
|
Name of each exchange on which registered |
| Common Stock, par value $0.001 per share |
|
SVRA |
|
The Nasdaq Global Select Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in as defined in Rule 405 of the Securities Act of 1933 (§ 230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§ 240.12b-2 of this chapter).
Emerging growth company ☐
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
| Item 7.01. |
Regulation FD Disclosure. |
Savara has updated its corporate presentation, which is available on the Investor Relations page of Savara’s website at https://savarapharma.com/investors/events-presentations/. A copy of the presentation is furnished as Exhibit 99.1 to this Current Report on Form 8-K. Savara undertakes no duty or obligation to update or revise the information contained in this presentation, although it may do so from time to time. Any such updates may be made through the Investor Relations page of the Savara website, the filing of other reports or documents with the U.S. Securities and Exchange Commission (the “SEC”), press releases, or other public disclosure.
The information in Item 7.01 in this Current Report on Form 8-K shall not be deemed “filed” for purposes of Section 18 of the Exchange Act, or otherwise subject to the liabilities of that Section, nor shall it be incorporated by reference in any filing under the Securities Act of 1933, as amended, or the Exchange Act, except as shall be expressly set forth by specific reference in such filing.
| Item 9.01. |
Financial Statements and Exhibits. |
(d) Exhibits.
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
|
|
|
|
|
| Date: January 5, 2024 |
|
|
|
SAVARA INC. a Delaware corporation |
|
|
|
|
|
By: |
|
/s/ Dave Lowrance |
|
|
|
|
Dave Lowrance Chief Financial & Administrative Officer |

Exhibit 99.1 Corporate Overview Developing New Therapies for Rare
Respiratory Diseases January 2024
Safe Harbor Statement Savara Inc. (“Savara” or the
“Company”) cautions you that statements in this presentation that are not a description of historical fact are forward-looking statements which may be identified by the use of words such as “expect,” “intend,”
“plan,” “anticipate,” “believe,” and “will,” among others. Such statements include, but are not limited to, statements regarding the nature, strategy and focus of Savara; the Savara investment thesis;
the timing, design and other matters related to clinical trials of our product candidate; the safety, efficacy and projected development timeline of our product candidate; the potential health benefits of our product candidate; our anticipated
corporate milestones; the potential market size, commercial opportunity, and competitive landscape for our product; Savara’s disease awareness campaign and GM-CSF autoantibody testing, and the potential impact of those programs; and the
sufficiency of our resources to fund the advancement of our development program and potential sources of additional capital. Savara may not actually achieve any of its plans or product development goals in a timely manner, if at all, or otherwise
carry out its current intentions or meet the expectations or projections disclosed in its forward-looking statements, and you should not place undue reliance on these forward-looking statements. Because such statements are subject to risks and
uncertainties, actual results may differ materially from those expressed or implied by such forward-looking statements. These forward-looking statements are based upon Savara's current expectations and involve assumptions that may never materialize
or may prove to be incorrect. Actual results and the timing of events could differ materially from those anticipated in such forward-looking statements as a result of various risks and uncertainties, which include, without limitation, the risks and
uncertainties related to the impact of widespread health concerns impacting healthcare providers or patients and geopolitical conditions on our business and operations; risks and uncertainties associated with the ability to project future cash
utilization and reserves needed for contingent future liabilities and business operations; the availability of sufficient resources for our operations and to conduct or continue planned clinical development programs; the timing and ability of Savara
to raise additional capital as needed to fund continued operations; the ability to successfully conduct clinical trials for our product candidate; the ability to successfully develop our product candidate; and the risks associated with the process
of developing, obtaining regulatory approval for and commercializing drug candidates that are safe and effective for use as human therapeutics. The risks and uncertainties facing Savara are described more fully in Savara's filings with the
Securities and Exchange Commission including our filings on Form 8-K, our Annual Report on Form 10-K for the fiscal year ended December 31, 2022, and our Quarterly Report on Form 10-Q for the quarter ended Sept. 30, 2023. You are cautioned not to
place undue reliance on our forward-looking statements, which speak only as of the date on which they were made. Savara undertakes no obligation to update such statements to reflect events that occur or circumstances that exist after the date on
which they were made, except as may be required by law. Third-party information included herein has been obtained from sources believed to be reliable, but the accuracy or completeness of such information is not guaranteed by, and should not be
construed as a representation by, the Company. The trademarks included herein are the property of the owners thereof and are used for reference purposes only. Such use should not be construed as an endorsement of such products. 2 © Savara Inc.
All Rights Reserved.

Executive Leadership Team Matthew Pauls, J.D., M.B.A. Chair & Chief
Executive Officer Ray Pratt, M.D. FACP Anne Erickson Dave Lowrance Rob Lutz, M.B.A. Chief Medical Officer Chief Business Officer Chief Financial & Administrative Officer Chief Operating Officer Scott Wilhoit Yasmine Wasfi, M.D., Ph.D. EVP,
Global Commercial SVP, Head of Clinical Development 3 © Savara Inc. All Rights Reserved.

Single Phase 3 program with high probability of success Investment
Thesis – Top line data expected end of 2Q24: ▪ Molgramostim nebulizer solution (molgramostim) in autoimmune pulmonary alveolar proteinosis (aPAP) ▪ Favorable efficacy and safety data generated from the first IMPALA trial ▪
Pivotal Phase 3 trial underway • Builds on key learnings from IMPALA Strong global commercial opportunity ▪ Significant unmet need – potential to be first and only approved treatment for aPAP globally ▪ Chronic dosing
expected ▪ Market expansion opportunities As a novel inhaled biologic, molgramostim has: ▪ 12-year biologic exclusivity in U.S. ▪ Potential for a long-term, durable revenue stream with biosimilar competition unlikely 4 ©
Savara Inc. All Rights Reserved.

Molgramostim Key Highlights 2012 2022 2020 Molgramostim granted Orphan
Drug UK’s Medicines and Healthcare Products Designation IMPALA results published in New Regulatory Agency (MHRA) awarded England Journal of Medicine molgramostim Innovation Passport and Promising Innovative Medicine Designations 2019
Molgramostim granted Fast Track Designation for aPAP 2021 2023 IMPALA-2 first patient dosed IMPALA-2 prespecified DMC* #2: Positive review Molgramostim granted IMPALA-2 Breakthrough Therapy prespecified DMC* Designation for aPAP #1: Positive review
IMPALA top IMPALA-2 line results enrollment completed (n=164, target was 160) Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 *The Data Monitoring Committee (DMC) conducted two pre-planned evaluations of IMPALA-2 to assess safety and
sample size. In both cases the DMC recommended that the study continue unmodified. 5
Molgramostim Molgramostim for Autoimmune Pulmonary Alveolar Proteinosis
(aPAP)

aPAP: An Autoimmune Disease of Alveolar Macrophage Dysfunction GM-CSF
Autoantibodies GM-CSF Normal Alveolus Alveolus in PAP NORMAL LUNG aPAP FUNCTION Thin surfactant layer Thick surfactant layer Rare lung disease caused by GM-CSF Alveoli need surfactant to keep autoantibodies which block from collapsing Alveolar
epithelial cells GM-CSF signaling and GM-CSF reduce surfactant clearance. GM-CSF GM-CSF is critical for alveolar GM-CSF This results in: autoantibodies macrophage function and allows for alveolar surfactant homeostasis, Surfactant accumulation that
structure, function, and host defense Foamy blocks movement of oxygen from alveolar the alveoli into the blood Normal macrophage alveolar (lipid filled) macrophage Normal Reduced blood oxygenation that Reduced oxygen delivery makes it hard to breath
and, oxygen delivery ultimately, hypoxemic respiratory Air-filled alveolus Surfactant-filled alveolus failure 7 © Savara Inc. All Rights Reserved.
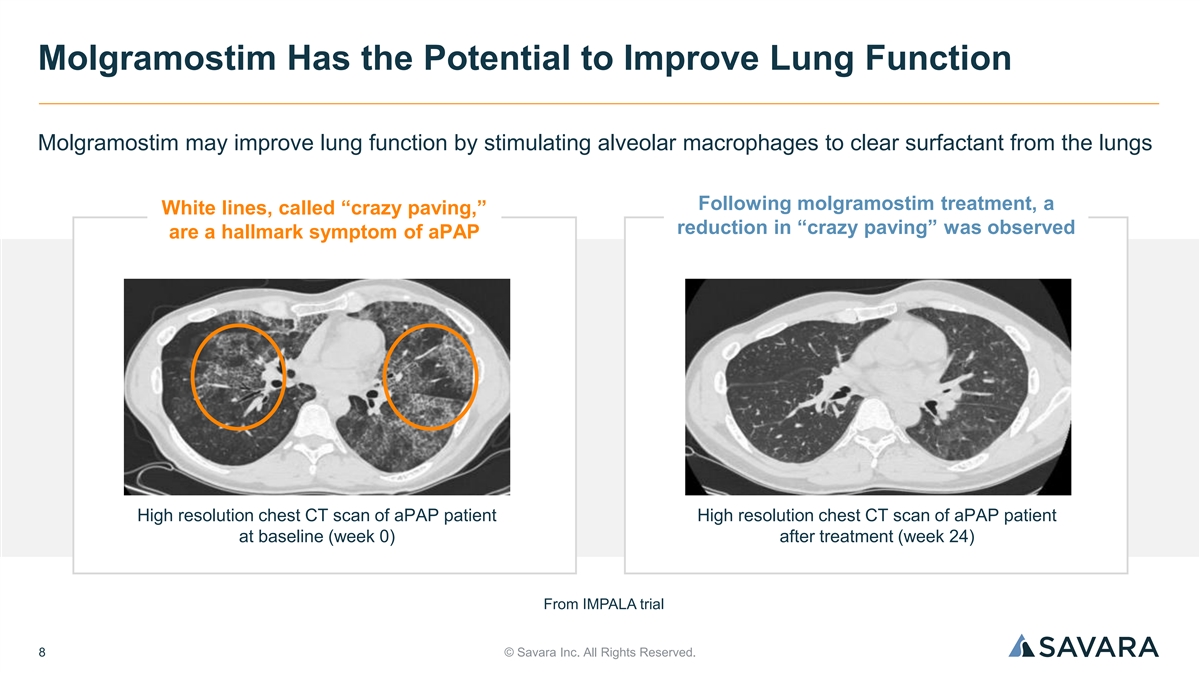
Molgramostim Has the Potential to Improve Lung Function Molgramostim may
improve lung function by stimulating alveolar macrophages to clear surfactant from the lungs Following molgramostim treatment, a White lines, called “crazy paving,” reduction in “crazy paving” was observed are a hallmark
symptom of aPAP High resolution chest CT scan of aPAP patient High resolution chest CT scan of aPAP patient at baseline (week 0) after treatment (week 24) From IMPALA trial 8 © Savara Inc. All Rights Reserved.

aPAP is a Rare, Long-Term, Chronic Disease Progressive Shortness of
Breath Fatigue, Decreased Exercise Tolerance ▪ Fatigue and significantly reduced exercise capacity can ▪ Gas exchange in the lungs is impaired and dramatically impact the simplest of daily activities, e.g., patients may experience
shortness of breath getting winded walking up a flight of stairs ▪ At first it occurs upon exertion, but as disease progresses, it can occur even when a person is at rest Cough and Episodes of Fever Fibrosis and Lung Transplant ▪ Cough,
sputum production, and episodes of fever, ▪ In the long-term, the disease can lead to serious especially if secondary lung infection develops complications, including fibrosis, and may lead to the need for lung transplantation There are no
approved drugs for the treatment of aPAP. Only option is whole lung lavage, an invasive procedure. 9 © Savara Inc. All Rights Reserved.

Unmet Need: aPAP Patients Have Significantly Higher Rates of 1
Healthcare Utilization and Comorbidities Charlson Outpatient visits Comorbidity Index +66% 3.5x (~17 per year) (CCI)* Vs. Vs. matched matched controls controls PAP: 1.84 ± 2.48 PAP: 17.30 ± 13.77 Age and Gender Matched Controls: 0.55
± 1.44 Age and Gender Matched Controls: 10.40 ± 11.38 P value: <0.0001 P value: <0.01 *Developed to classify comorbid conditions which may influence mortality risk. Most widely used comorbidity index used to determine survival rates
in patients with multiple comorbidities. Longer hospital stays Emergency Room Visits +38% 3.0x (~16 days per year) (~1.5 per year) Vs. Vs. matched matched controls controls PAP: 1.49 ± 1.17 PAP: 15.96 ± 20.71 Age and Gender Matched
Controls: 1.08 ± 0.27 Age and Gender Matched Controls: 5.40 ± 5.07 P value: 0.014 P value: 0.027 10 © Savara Inc. All Rights Reserved. 1: McCarthy et al. Orphanet Journal of Rare Diseases (2018) 13:129
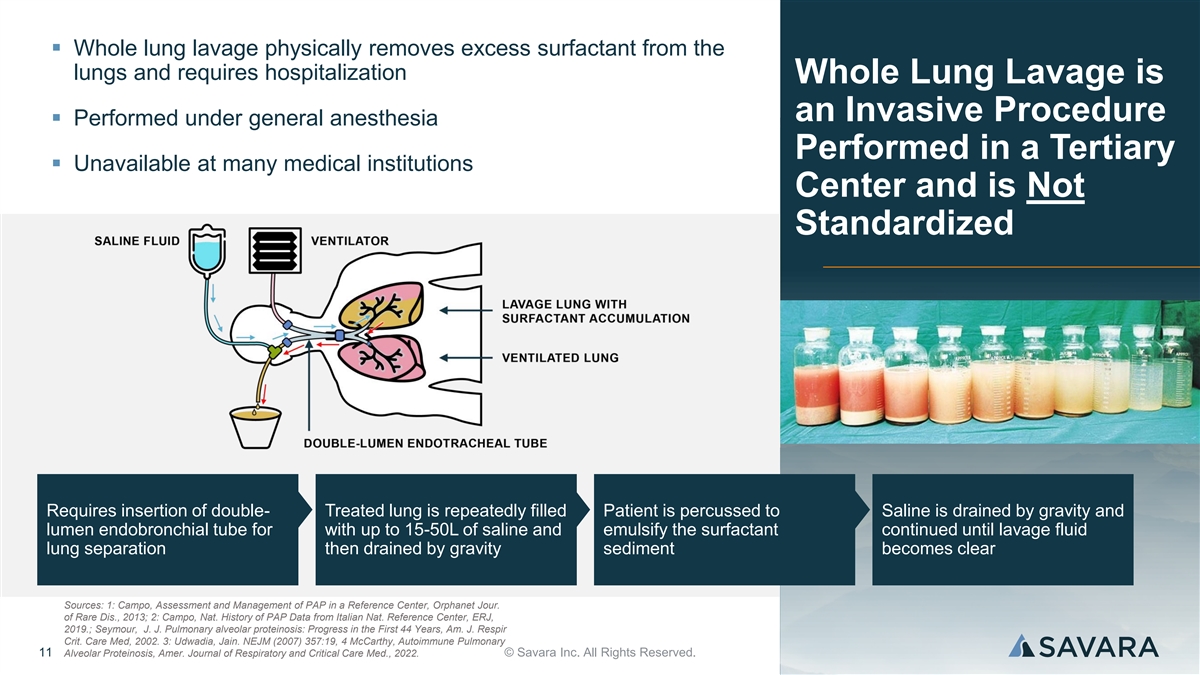
▪ Whole lung lavage physically removes excess surfactant from the
lungs and requires hospitalization Whole Lung Lavage is an Invasive Procedure ▪ Performed under general anesthesia Performed in a Tertiary ▪ Unavailable at many medical institutions Center and is Not Standardized Requires insertion of
double- Treated lung is repeatedly filled Patient is percussed to Saline is drained by gravity and lumen endobronchial tube for with up to 15-50L of saline and emulsify the surfactant continued until lavage fluid lung separation then drained by
gravity sediment becomes clear Sources: 1: Campo, Assessment and Management of PAP in a Reference Center, Orphanet Jour. of Rare Dis., 2013; 2: Campo, Nat. History of PAP Data from Italian Nat. Reference Center, ERJ, 2019.; Seymour, J. J. Pulmonary
alveolar proteinosis: Progress in the First 44 Years, Am. J. Respir Crit. Care Med, 2002. 3: Udwadia, Jain. NEJM (2007) 357:19, 4 McCarthy, Autoimmune Pulmonary 11 Alveolar Proteinosis, Amer. Journal of Respiratory and Critical Care Med., 2022.
© Savara Inc. All Rights Reserved.
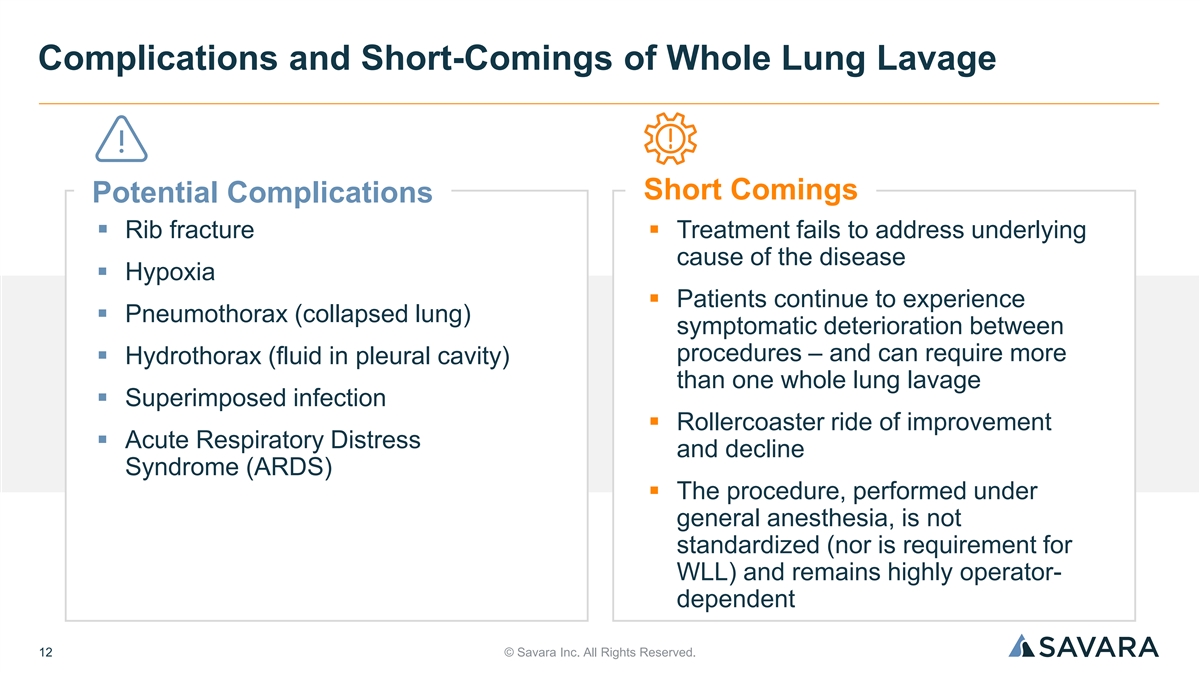
Complications and Short-Comings of Whole Lung Lavage Short Comings
Potential Complications ▪ Rib fracture▪ Treatment fails to address underlying cause of the disease ▪ Hypoxia ▪ Patients continue to experience ▪ Pneumothorax (collapsed lung) symptomatic deterioration between procedures
– and can require more ▪ Hydrothorax (fluid in pleural cavity) than one whole lung lavage ▪ Superimposed infection ▪ Rollercoaster ride of improvement ▪ Acute Respiratory Distress and decline Syndrome (ARDS) ▪ The
procedure, performed under general anesthesia, is not standardized (nor is requirement for WLL) and remains highly operator- dependent 12 © Savara Inc. All Rights Reserved.

Historically, Without a Broadly Available Diagnostic for aPAP, the
Journey to Diagnosis Can Be Long and Misdiagnosis Common 1 ▪ 3-36 months : Range for aPAP time-to- diagnosis 4 U.S. National PAP Registry indicates many patients 2 ▪ 18 months : Average delay caused by with PAP are diagnosed via an
invasive misdiagnosis (e.g., pneumonia or asthma) transbronchial biopsy, surgical lung biopsy, or 3 both ▪ Diagnostic workup frequently involves multiple tests and invasive procedures, including Transbronchial • Pulmonary function tests
Surgical Biopsy Biopsy 30% 29% • Arterial blood gas analysis • Chest radiographs • CT scans Surgical plus • Bronchoalveolar lavage (BAL) cytology and/or lung Transbronchial No Biopsy 3 Biopsy histopathology 18% 23% •
Transbronchial biopsy, surgical lung biopsy, or both Sources: 1: Campo Orphanet J Rare Dis 2013; 2: Trapnell Nat Rev Dis Primers 2019; 3: McCarthy Chest 2019; 4: Trapnell PAP Registry http://clinicaltrials.gov/ct2/show/ 13 © Savara Inc. All
Rights Reserved.

Savara Investigational Drug-Device Treatment for aPAP Molgramostim
nebulization time = 3-5 minutes ▪ Once daily 300 µg inhaled molgramostim ▪ Proprietary Pari eFlow® Nebulizer System • Optimized for molgramostim administration • Well-established manufacturer of devices used for
inhalation therapy • Pari has 5 FDA approved nebulizers 14 © Savara Inc. All Rights Reserved.
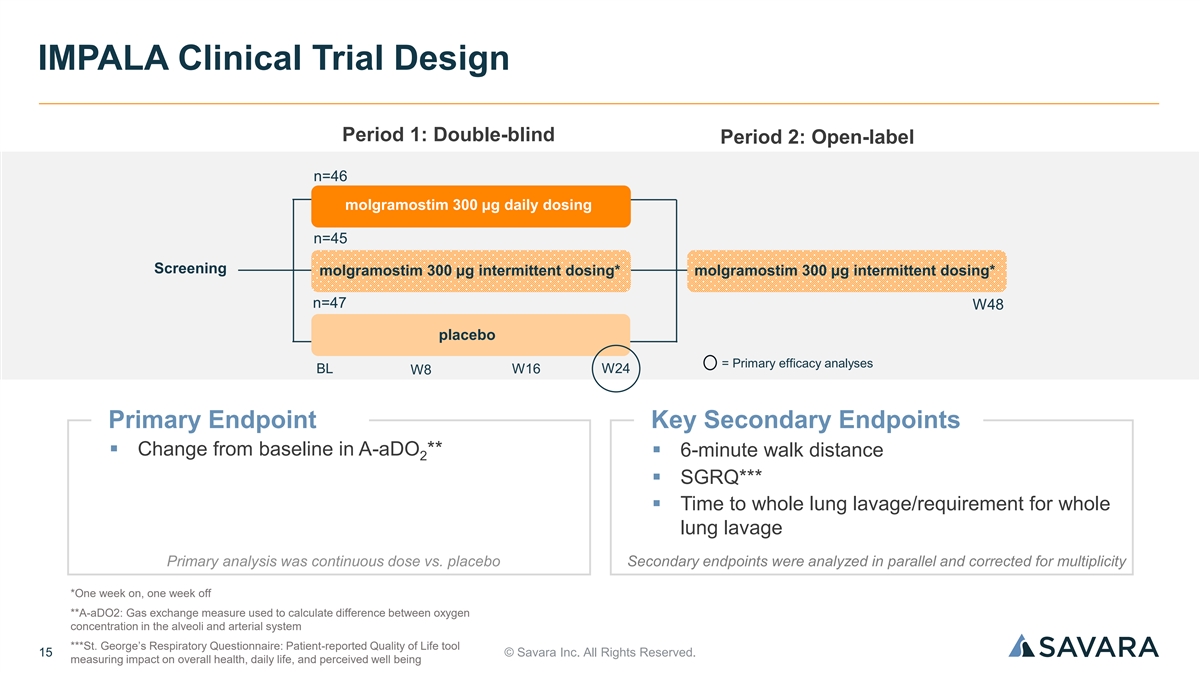
IMPALA Clinical Trial Design Period 1: Double-blind Period 2:
Open-label n=46 molgramostim 300 μg daily dosing n=45 Screening molgramostim 300 μg intermittent dosing* molgramostim 300 μg intermittent dosing* n=47 W48 placebo = Primary efficacy analyses BL W16 W24 W8 Primary Endpoint Key
Secondary Endpoints ▪ Change from baseline in A-aDO **▪ 6-minute walk distance 2 ▪ SGRQ*** ▪ Time to whole lung lavage/requirement for whole lung lavage Primary analysis was continuous dose vs. placebo Secondary endpoints
were analyzed in parallel and corrected for multiplicity *One week on, one week off **A-aDO2: Gas exchange measure used to calculate difference between oxygen concentration in the alveoli and arterial system ***St. George’s Respiratory
Questionnaire: Patient-reported Quality of Life tool 15 © Savara Inc. All Rights Reserved. measuring impact on overall health, daily life, and perceived well being

IMPALA Trial Did Not Meet the Primary Endpoint Continuous Once Daily
(QD) Dosing Regimen 1 Full Analysis Set (FAS)* Estimated treatment difference of -4.6 mmHg (p=0.17) Revised FAS** Estimated treatment difference of -6.5 mmHG (p=0.025) *Protocol specified analysis (ITT). **Revised analysis excluded 4 patients using
supplemental oxygen during testing (placebo: n=2, intermittent: n=1, continuous: n=1). 16 1: Trapnell, Inhaled Molgramostim Therapy in aPAP, NEJM, 2020. © Savara Inc. All Rights Reserved.

IMPALA: DLCO and SGRQ Showed Robust Improvement with Continuous Once
Daily (QD) Dosing Regimen Change in St. George’s Respiratory Questionnaire Change in Diffusion Capacity for Carbon Monoxide 1 1 (SGRQ) From Baseline Over 24-weeks (FAS) (DLCO) From Baseline Over 24-weeks (FAS) 1 20 0 16 -4 12 -8 8 -12 4 0 -16
0 4 8 12 16 20 24 0 4 12 24 Week Week QD estimated treatment difference of QD estimated treatment difference of 7.9% predicted (p=0.007) 7.6 points (p=0.01) Became Primary Endpoint in IMPALA-2 Became Key Secondary Endpoint in IMPALA-2 17 1:
Trapnell, Inhaled Molgramostim Therapy in aPAP, NEJM, 2020. © Savara Inc. All Rights Reserved. Results not adjusted for multiplicity. Mean Change (% Predicted) Mean Change (Score)

IMPALA Open-Label Data Showed Sustained Effect, or Continued
Improvement, after Longer-Term Drug Exposure Mean Change in DLCO Mean Change in SGRQ Total Score Use of Whole Lung Lavage During 1 1 1 Over Time Over Time the Blinded Treatment Period Blinded Period Open-Label Period 24 Hazard ratio for All patients
received All patients received Time to First Whole molgramostim intermittent molgramostim intermittent Lung Lavage vs 20 dosing dosing Placebo 16 12 Rate ratio for Frequency of Whole Lung Lavage 8 vs Placebo 4 0.01 0.1 1 10 100 0 0 8 16 24 36 48 60
72 Molgramostim Placebo n=44 n=43 n=40 n=19 Week Better Better n=46 n=42 n=41 n=18 Continuous molgramostim Placebo Intermittent molgramostim Dosing schedules for blinded and open-label periods were different. 18 1: Trapnell, Inhaled Molgramostim
Therapy in aPAP, NEJM, 2020. © Savara Inc. All Rights Reserved. Mean Change (% Predicted)

IMPALA Safety Overview % PATIENTS WITH ADVERSE EVENTS (AEs) DURING
DOUBLE-BLIND TREATMENT PERIOD* Category Continuous molgramostim Placebo (Patients with AEs >5% in double-blind treatment period) (n=46) (n=47) Any adverse event 84.8% 87.2% Most common adverse events Cough 32.6% 23.4% Chest pain 21.7% 2.1%
Nasopharyngitis 15.2% 12.8% Headache 13.0% 14.9% Dyspnea 10.9% 8.5% Productive cough 8.7% 6.4% Adverse events possibly or probably related to the intervention 32.6% 29.8% Adverse events leading to discontinuation of the intervention 4.3% 2.1%
*Trapnell, Inhaled Molgramostim Therapy in aPAP, NEJM Supplementary Appendix, 2020 19 © Savara Inc. All Rights Reserved.

Phase 3 IMPALA-2 Trial Design Leverages IMPALA Key Learnings Top Line
Data Expected End of 2Q24 Period 1: Double-blind Period 2: Open-label 6-Week Screening n=80 • DLCO ≤70% predicted molgramostim 300 μg daily dosing at first screening and baseline molgramostim 300 μg daily dosing • Change
in % predicted n=80 <15% points to ensure W144 stably impaired patients placebo BL = Primary efficacy analyses W24 W48 = Durability of efficacy / safety Primary Endpoint Secondary Endpoints ▪ Change from baseline in DLCO ▪ SGRQ Total
Score • 90% powered to detect 5.7% predicted ▪ SGRQ Activity Score difference with standard deviation of 11* ▪ Exercise capacity using treadmill test *Based on patient level data from IMPALA that best matches expected population
for IMPALA-2 20 © Savara Inc. All Rights Reserved.
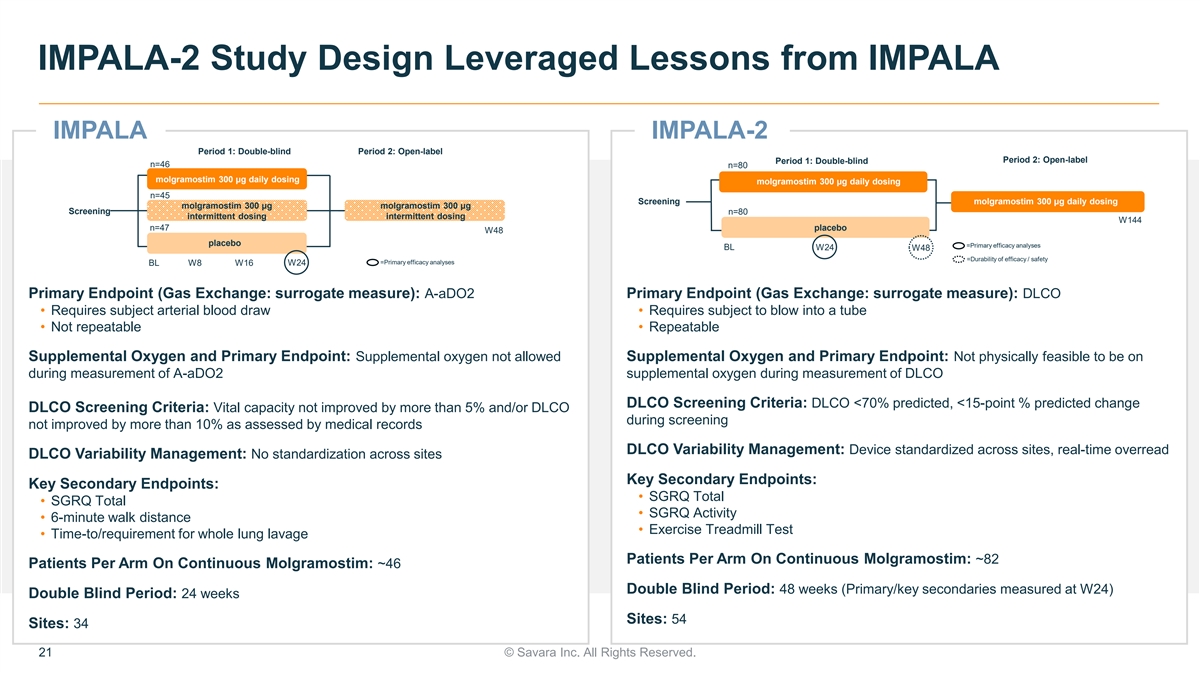
IMPALA-2 Study Design Leveraged Lessons from IMPALA IMPALA IMPALA-2
Period 1: Double-blind Period 2: Open-label Period 2: Open-label Period 1: Double-blind n=46 n=80 molgramostim 300 μg daily dosing molgramostim 300 μg daily dosing n=45 Screening molgramostim 300 μg daily dosing molgramostim 300
μg molgramostim 300 μg Screening n=80 intermittent dosing intermittent dosing W144 n=47 placebo W48 placebo =Primary efficacy analyses BL W24 W48 =Durability of efficacy / safety =Primary efficacy analyses BL W8 W16 W24 Primary Endpoint
(Gas Exchange: surrogate measure): A-aDO2 Primary Endpoint (Gas Exchange: surrogate measure): DLCO • Requires subject arterial blood draw • Requires subject to blow into a tube • Not repeatable • Repeatable Supplemental
Oxygen and Primary Endpoint: Supplemental oxygen not allowed Supplemental Oxygen and Primary Endpoint: Not physically feasible to be on during measurement of A-aDO2 supplemental oxygen during measurement of DLCO DLCO Screening Criteria: DLCO <70%
predicted, <15-point % predicted change DLCO Screening Criteria: Vital capacity not improved by more than 5% and/or DLCO during screening not improved by more than 10% as assessed by medical records DLCO Variability Management: Device
standardized across sites, real-time overread DLCO Variability Management: No standardization across sites Key Secondary Endpoints: Key Secondary Endpoints: • SGRQ Total • SGRQ Total • SGRQ Activity • 6-minute walk distance
• Exercise Treadmill Test • Time-to/requirement for whole lung lavage Patients Per Arm On Continuous Molgramostim: ~82 Patients Per Arm On Continuous Molgramostim: ~46 Double Blind Period: 48 weeks (Primary/key secondaries measured at
W24) Double Blind Period: 24 weeks Sites: 54 Sites: 34 21 © Savara Inc. All Rights Reserved.
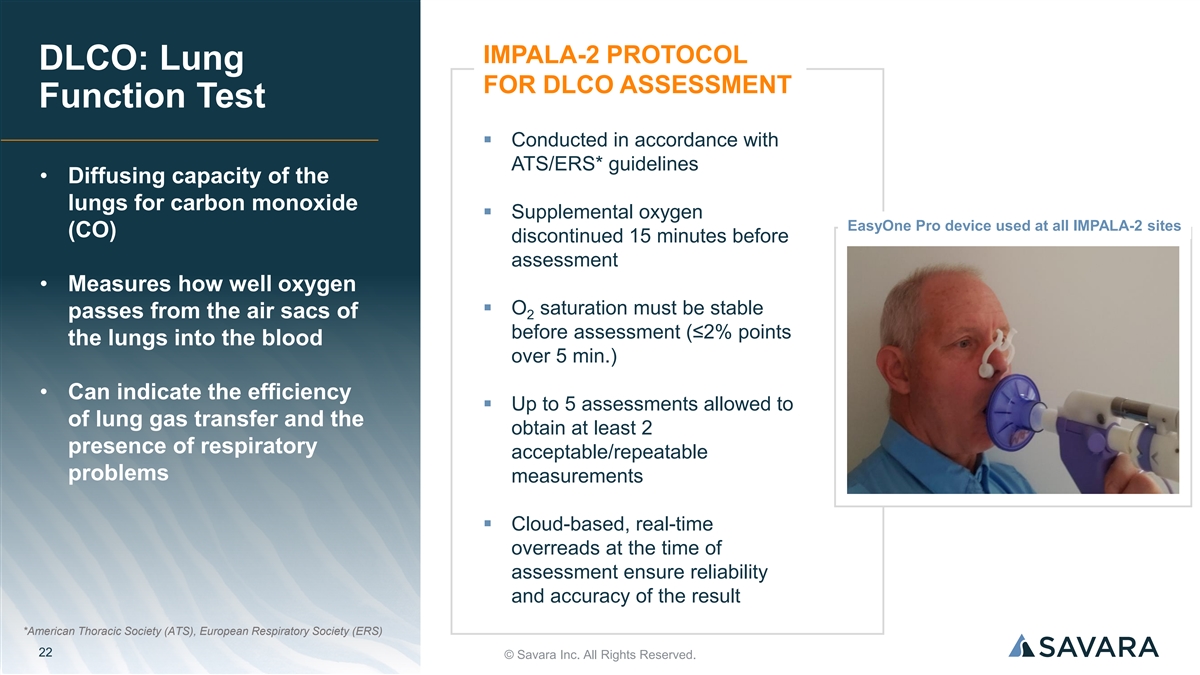
IMPALA-2 PROTOCOL DLCO: Lung FOR DLCO ASSESSMENT Function Test ▪
Conducted in accordance with ATS/ERS* guidelines • Diffusing capacity of the lungs for carbon monoxide ▪ Supplemental oxygen EasyOne Pro device used at all IMPALA-2 sites (CO) discontinued 15 minutes before assessment • Measures
how well oxygen ▪ O saturation must be stable passes from the air sacs of 2 before assessment (≤2% points the lungs into the blood over 5 min.) • Can indicate the efficiency ▪ Up to 5 assessments allowed to of lung gas
transfer and the obtain at least 2 presence of respiratory acceptable/repeatable problems measurements ▪ Cloud-based, real-time overreads at the time of assessment ensure reliability and accuracy of the result *American Thoracic Society (ATS),
European Respiratory Society (ERS) 22 © Savara Inc. All Rights Reserved.

MOLGRAMOSTIM IN aPAP REGULATORY DESIGNATIONS ▪ Orphan Drug
Designation, Europe (eligible for 10 years exclusivity) ▪ Orphan Drug Designation, U.S. (eligible for 7 years exclusivity) Molgramostim ▪ Fast Track Designation, U.S. ▪ Breakthrough Therapy Designation, U.S. Regulatory ▪
Innovation Passport Designation, U.K. Landscape ▪ Promising Innovative Medicine Designation, U.K. IMPALA-2 ▪ Trial design endorsed by regulatory authorities in the U.S., Canada, Japan, South Korea, Australia, U.K., and countries in
Europe where the trial is being conducted BIOLOGIC EXCLUSIVITY ▪ Upon Biologics License Application (BLA) approval FDA would grant 12 years marketing exclusivity 23 © Savara Inc. All Rights Reserved.

Commercial Outlook

aPAP Diagnosed Prevalence Before and After Broad Availability of GM-CSF
Autoantibody Testing Published aPAP Epidemiology Studies DIAGNOSED IMPLIED IMPLIED IMPLIED TOTAL INCIDENCE Current REFERENCE METHODOLOGY PREVALENCE US EU JAPAN IMPLIED PER MILLION Diagnosed PER MILLION PATIENTS PATIENTS PATIENTS PATIENTS Prevalence
DIAGNOSED PREVALENCE Before Broad GM-CSF Registry based in 0.48 6.2 Inoue 2008 ~2,058 ~2,325 ~775 ~5,158 Autoantibody Niigata, Japan (0.23-1.00) (3.8-10.3) Testing US insurance claims 6.3 McCarthy 2018 Not reported ~2,092 ~2,363 ~788 ~5,243 data,
2008-2012 (5.2-7.6) DIAGNOSED IMPLIED IMPLIED TOTAL INCIDENCE IMPLIED EU Diagnosed REFERENCE METHODOLOGY PREVALENCE US JAPAN IMPLIED PER MILLION PATIENTS Prevalence After PER MILLION PATIENTS PATIENTS PATIENTS Broad GM-CSF DIAGNOSED PREVALENCE
Autoantibody Testing Update of Niigata 1.66 26.6 Kitamura 2019 ~8,831 ~9,975 ~3,325 ~22,131 registry (1.2-2.2) (9.0-73.0) CONFIDENTIAL 25 © Savara Inc. All Rights Reserved.

Re-analysis of Claims Dataset Estimates There Are ~5,000 aPAP Patients
in the U.S. ANALYSIS OF COMPREHENSIVE CLAIMS DATASET Real-World Claims Dataset: ~3,600* ▪ 300M+ unique, active patients U.S. patients with at least 1 ▪ 89-99% providers/sites of care PAP ICD9/10 diagnosis code in claims history ▪
Counted PAP ICD9/10 diagnosis claims ~5,000 estimated aPAP patients in the U.S., based on identified PAP claims APPLIED MACHINE LEARNING (ML) history and machine MODEL TO SAME CLAIMS DATASET learning assessment ML model identified patients who have
high likelihood of PAP, but are not yet diagnosed (patients were required to have either a bronchoscopy, BAL, or lung lavage in their claims history) *Data from 2023 U.S. insurance claims analysis conducted by Savara. Highly likely patients: ≥
2 PAP diagnosis claims, likely patients: 1 PAP diagnosis claim CONFIDENTIAL 26 © Savara Inc. All Rights Reserved.

December 2023: Launched HCP Disease Awareness Campaign and No-Cost
GM-CSF Autoantibody Testing in U.S. 1,111 affiliated accounts* with ≥2 aPAP diagnosis claims ~5K ~15K HCPs with diagnosed or machine- Pulmonologists in the US learning suspected PAP patients ~10 ~120 PAP clinical centers Pulmonology centers
Patient Advocacy Group www.apapclearpath.com U.S. HCP Website Partnerships/Memberships ▪ Increase HCP awareness of aPAP, including hallmark symptoms of the disease ▪ Educate HCPs on need for routine GM-CSF autoantibody testing ▪
REQUEST THE TEST: Order a simple, non-invasive, no-cost GM-CSF autoantibody blood test • *Any hospital and health system the diagnosing HCP is affiliated with (within the U.S. claims database). • Data on file. 27 © Savara Inc. All
Rights Reserved.

Molgramostim: Global Commercial Opportunity Significant Unmet Need
Molgramostim ▪ High disease burden▪ Potential first and only approved treatment for aPAP globally – WLL (standard of care) is invasive and ▪ Strong market expansion not standardized potential via disease awareness campaign,
broad access to GM-CSF ▪ Dosing expected to be chronic, autoantibody testing providing long-term revenue stream ▪ Assumed pricing power consistent with analogous Significant orphan drug biologics Commercial Opportunity Rare Disease
Infrastructure Long Term Exclusivity ▪ Orphan disease-like ▪ 12-year biologic exclusivity in infrastructure in U.S. – field-based the U.S. and biosimilar team of ~15-30 competition unlikely ▪ OUS commercial strategy
optionality – go-it-alone, regional partnerships, etc. *Compared to matched controls. Data on file 28 © Savara Inc. All Rights Reserved.

Financials
▪ Well capitalized into 2026 • ~$168M in cash* ▪
Strong investor support with coverage from Financial 6 equity research analysts Highlights ANALYST COVERAGE Evercore ISI Liisa Bayko, MSC, MBA Guggenheim Securities Vamil Divan, MD, MBA H.C. Wainwright Andrew Fein Jefferies Andrew Tsai Oppenheimer
Francois Brisebois Piper Sandler Yasmeen Rahimi, PhD 30 *Cash, cash equivalents, and short-term investments as of 9/30/23 © Savara Inc. All Rights Reserved.

Single Phase 3 program with high probability of success Investment
Thesis – Top line data expected end of 2Q24: ▪ Molgramostim nebulizer solution (molgramostim) in autoimmune pulmonary alveolar proteinosis (aPAP) ▪ Favorable efficacy and safety data generated from the first IMPALA trial ▪
Pivotal Phase 3 trial underway • Builds on key learnings from IMPALA Strong global commercial opportunity ▪ Significant unmet need – potential to be first and only approved treatment for aPAP globally ▪ Chronic dosing
expected ▪ Market expansion opportunities As a novel inhaled biologic, molgramostim has: ▪ 12-year biologic exclusivity in U.S. ▪ Potential for a long-term, durable revenue stream with biosimilar competition unlikely 31 ©
Savara Inc. All Rights Reserved.

Thank You
v3.23.4
| X |
- DefinitionBoolean flag that is true when the XBRL content amends previously-filed or accepted submission.
| Name: |
dei_AmendmentFlag |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionFor the EDGAR submission types of Form 8-K: the date of the report, the date of the earliest event reported; for the EDGAR submission types of Form N-1A: the filing date; for all other submission types: the end of the reporting or transition period. The format of the date is YYYY-MM-DD.
| Name: |
dei_DocumentPeriodEndDate |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:dateItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe type of document being provided (such as 10-K, 10-Q, 485BPOS, etc). The document type is limited to the same value as the supporting SEC submission type, or the word 'Other'.
| Name: |
dei_DocumentType |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:submissionTypeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 1 such as Attn, Building Name, Street Name
| Name: |
dei_EntityAddressAddressLine1 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 2 such as Street or Suite number
| Name: |
dei_EntityAddressAddressLine2 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- Definition
+ References
+ Details
| Name: |
dei_EntityAddressCityOrTown |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCode for the postal or zip code
| Name: |
dei_EntityAddressPostalZipCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the state or province.
| Name: |
dei_EntityAddressStateOrProvince |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:stateOrProvinceItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionA unique 10-digit SEC-issued value to identify entities that have filed disclosures with the SEC. It is commonly abbreviated as CIK. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityCentralIndexKey |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:centralIndexKeyItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionIndicate if registrant meets the emerging growth company criteria. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityEmergingGrowthCompany |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCommission file number. The field allows up to 17 characters. The prefix may contain 1-3 digits, the sequence number may contain 1-8 digits, the optional suffix may contain 1-4 characters, and the fields are separated with a hyphen.
| Name: |
dei_EntityFileNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:fileNumberItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTwo-character EDGAR code representing the state or country of incorporation.
| Name: |
dei_EntityIncorporationStateCountryCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarStateCountryItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe exact name of the entity filing the report as specified in its charter, which is required by forms filed with the SEC. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityRegistrantName |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe Tax Identification Number (TIN), also known as an Employer Identification Number (EIN), is a unique 9-digit value assigned by the IRS. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityTaxIdentificationNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:employerIdItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionLocal phone number for entity.
| Name: |
dei_LocalPhoneNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 13e
-Subsection 4c
| Name: |
dei_PreCommencementIssuerTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 14d
-Subsection 2b
| Name: |
dei_PreCommencementTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTitle of a 12(b) registered security. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b
| Name: |
dei_Security12bTitle |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:securityTitleItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the Exchange on which a security is registered. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection d1-1
| Name: |
dei_SecurityExchangeName |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarExchangeCodeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as soliciting material pursuant to Rule 14a-12 under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Section 14a
-Number 240
-Subsection 12
| Name: |
dei_SolicitingMaterial |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTrading symbol of an instrument as listed on an exchange.
| Name: |
dei_TradingSymbol |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:tradingSymbolItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as written communications pursuant to Rule 425 under the Securities Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Securities Act
-Number 230
-Section 425
| Name: |
dei_WrittenCommunications |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
Savara (NASDAQ:SVRA)
Historical Stock Chart
From Mar 2024 to Apr 2024

Savara (NASDAQ:SVRA)
Historical Stock Chart
From Apr 2023 to Apr 2024
