false 0001796280 0001796280 2024-01-09 2024-01-09
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of The Securities Exchange Act of 1934
Date of Report (Date of earliest event reported)
January 9, 2024
ORIC Pharmaceuticals, Inc.
(Exact name of registrant as specified in its charter)
|
|
|
|
|
| Delaware |
|
001-39269 |
|
47-1787157 |
| (State or other jurisdiction of incorporation) |
|
(Commission File Number) |
|
(IRS Employer Identification No.) |
240 E. Grand Ave, 2nd Floor
South San Francisco, CA 94080
(Address of principal executive offices, including zip code)
(650) 388-5600
(Registrant’s telephone number, including area code)
Not Applicable
(Former name or former address, if changed since last report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| ☐ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ☐ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ☐ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ☐ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
|
|
|
|
|
| Title of each class |
|
Trading Symbol(s) |
|
Name of each exchange on which registered |
| Common stock, par value $0.0001 per share |
|
ORIC |
|
The Nasdaq Global Select Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company ☒
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☒
| Item 2.02 |
Results of Operations and Financial Condition. |
The information set forth in Item 7.01 is hereby incorporated by reference into this Item 2.02.
| Item 7.01 |
Regulation FD Disclosure. |
ORIC Pharmaceuticals, Inc. (the “Company”) intends to present an updated corporate presentation (the “Corporate Presentation”) at the 42nd Annual J.P. Morgan Healthcare Conference on January 9, 2024. A copy of the Corporate Presentation is furnished as Exhibit 99.1 hereto and is incorporated herein by reference.
All of the information furnished in this Item 7.01 and Items 2.02 and 9.01 (including Exhibit 99.1) shall not be deemed to be “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), or otherwise subject to the liabilities of that section, nor shall it be deemed incorporated by reference into any filing under the Securities Act of 1933, as amended, or the Exchange Act, except as shall be expressly set forth by specific reference in such a filing.
| Item 9.01 |
Financial Statements and Exhibits. |
(d) Exhibits.
|
|
|
| Exhibit Number |
|
Description |
|
|
| 99.1 |
|
Corporate Presentation |
|
|
| 104 |
|
Cover Page Interactive Data File (embedded within the Inline XBRL document) |
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
|
|
|
|
|
|
|
|
|
|
|
|
|
ORIC PHARMACEUTICALS, INC. |
|
|
|
|
| Date: January 9, 2024 |
|
|
|
By: |
|
/s/ Christian Kuhlen |
|
|
|
|
|
|
Christian Kuhlen, M.D., J.D. |
|
|
|
|
|
|
General Counsel |

Exhibit 99.1 Company Overview January 2024

Forward-Looking Statements This presentation contains forward-looking
statements that involve substantial risks and uncertainties. All statements other than statements of historical facts contained in this presentation, including statements regarding ORIC Pharmaceuticals, Inc.’s (“ORIC”,
“we”, “us” or “our”) future financial condition, results of operations, business strategy and plans, and objectives of management for future operations, as well as statements regarding industry trends, are
forward-looking statements. In some cases, you can identify forward-looking statements by terminology such as “anticipate,” “believe,” “continue,” “could,” “estimate,” “expect,”
“intend,” “may,” “plan,” “potentially,” “predict,” “should,” “will” or the negative of these terms or other similar expressions. Forward-looking statements contained
in this presentation also include, but are not limited to, statements regarding: our development plans and timelines; the potential advantages of our product candidates and programs; plans for the clinical trials and development of ORIC-114,
ORIC-944 and ORIC-533; the expected timing of reporting data from our clinical trials; our anticipated milestones and clinical updates; and the period over which we estimate our existing cash and investments will be sufficient to fund our current
operating plan. We have based these forward-looking statements largely on our current expectations and projections about future events and trends that we believe may affect our financial condition, results of operations, business strategy and
financial needs. These forward-looking statements are subject to a number of risks, uncertainties and assumptions, including, among other things: the timing of the initiation, progress and results of our preclinical studies and clinical trials;
risks associated with the process of discovering, developing and commercializing drugs that are safe and effective for use in humans and operating as an early clinical stage company; negative impacts of the COVID-19 pandemic on our operations,
including clinical trials; the potential for current or future clinical trials of product candidates to differ from preclinical, initial, interim, preliminary or expected results; our ability to advance product candidates into, and successfully
complete, clinical trials; the timing or likelihood of regulatory filings and approvals; changes in our plans to develop and commercialize our product candidates; our estimates of the number of patients who suffer from the diseases we are targeting
and the number of patients that may enroll in our clinical trials; the commercializing of our product candidates, if approved; our ability to successfully manufacture and supply our product candidates for clinical trials and for commercial use, if
approved; potential benefits and costs of strategic arrangements, licensing and/or collaborations; the risk of the occurrence of any event, change or other circumstance that could give rise to the termination of our license or collaboration
agreements; our estimates regarding expenses, future revenue, capital requirements and needs for financing and our ability to obtain capital; the sufficiency of our existing cash and investments to fund our future operating expenses and capital
expenditure requirements; our ability to retain the continued service of our key personnel and to identify, hire and retain additional qualified professionals; the implementation of our business model and strategic plans for our business and product
candidates; the scope of protection we are able to establish and maintain for intellectual property rights, product candidates and our pipeline; our ability to contract with third-party contract research organizations, suppliers and manufacturers
and their ability to perform adequately; the pricing, coverage and reimbursement of our product candidates, if approved; developments relating to our competitors and our industry, including competing product candidates and therapies; general
economic and market conditions; and the other risks, uncertainties and assumptions discussed in the public filings we have made and will make with the Securities and Exchange Commission (“SEC”). These risks are not exhaustive. New risk
factors emerge from time to time and it is not possible for our management to predict all risk factors, nor can we assess the impact of all factors on our business or the extent to which any factor, or combination of factors, may cause actual
results to differ materially from those contained in, or implied by, any forward-looking statements. You should not rely upon forward-looking statements as predictions of future events. Although we believe that the expectations reflected in the
forward-looking statements are reasonable, we cannot guarantee future results, levels of activity, performance or achievements. This presentation also contains estimates and other statistical data made by independent parties and by us relating to
market size and other data about our industry. This data involves a number of assumptions and limitations, and you are cautioned not to give undue weight to such data and estimates. In addition, projections, assumptions and estimates of our future
performance and the future performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk. Except as required by law, we undertake no obligation to update any statements in this presentation for any
reason after the date of this presentation. We have filed Current Reports on Form 8-K, Quarterly Reports on Form 10-Q, Annual Reports on Form 10-K, and other documents with the SEC. You should read these documents for more complete information about
us. You may obtain these documents for free by visiting EDGAR on the SEC website at www.sec.gov. This presentation discusses our product candidates that are under preclinical or clinical study, and which have not yet been approved for marketing by
the U.S. Food and Drug Administration. No representation is made as to the safety or effectiveness of our product candidates for the therapeutic use for which they are being studied. 2

ORIC Pharmaceuticals: Dedicated to Overcoming Resistance In Cancer
• Two potential best-in-class programs advancing towards pivotal studies Broad Pipeline of Potential First-in-Class and Best-in-Class Programs • Additional preclinical programs targeting novel and validated targets Precision Oncology
Expertise Enables • Rapid timelines enabled by biomarker-driven, patient-selected clinical Accelerated Clinical Timelines trials and translational expertise • Track record of building pipeline via internal R&D and business
development Dual Engines for Pipeline Expansion • Targeting one new IND candidate every 18 months • Heritage of discovering and developing multiple approved oncology medicines at Experienced Management Team Ignyta, Medivation, Aragon and
Genentech (1) Strong Financial Position • Cash and investments of $235 million expected to fund company into 2026 • ORIC-944 initiation of combination study with AR inhibitor(s): 1H 2024 • ORIC-944 program update: mid-2024
Anticipated Milestones • ORIC-114 initiation of dose expansion in multiple cohorts: 1H 2024 • ORIC-114 updated Phase 1b data: 1H 2025 (1) Approximate unaudited balance as of December 31, 2023. 3

Executive Team with Expertise in Building Leading Oncology Companies
• Previously CFO of Ignyta (acquired by Roche), raised over $500mm in capital Jacob Chacko, MD Chief Executive Officer • TPG Capital (completed $10bn of aggregate acquisitions) and McKinsey • Board member of 4D Molecular
Therapeutics and Board chair of Bright Peak Therapeutics; previously Turning Point, Bonti, RentPath, EnvisionRx, Par Pharma, IMS and Quintiles • Previously Head of Translational Oncology at Genentech; advanced over 20 drug candidates into Lori
Friedman, PhD development, two approvals to date Chief Scientific Officer • Director of Signal Transduction at Exelixis; led new target discovery collaboration with BMS • Inventor on 28 issued patents and author on 99 peer-reviewed
publications • Board member of NextRNA Therapeutics • Previously CMO of Ignyta, led development and regulatory for entrectinib Pratik Multani, MD Chief Medical Officer • CMO of Fate Therapeutics; contributed to development of
Rituxan and Zevalin at Idec, and Treanda at Salmedix; earlier at Dana Farber and MGH • Board member of Erasca and Chimerix • Previously SVP of Business Development at Prothena, established Celgene collaboration for up to $2.2bn Matt
Panuwat Chief Business Officer • Head of BD at Medivation (acquired by Pfizer), led M&A including the acquisition of talazoparib • Global Healthcare Investment Banking at Merrill Lynch • Previously CFO of AnaptysBio, raised
over $500mm in capital (IPO and follow-on financing) Dominic Piscitelli Chief Financial Officer • VP of Finance, Strategy and Investor Relations at Medivation • VP of Treasury and Finance at OSI Pharmaceuticals (acquired by Astellas)
• Board member of Celyad Oncology • Previously General Counsel at Synthorx (acquired by Sanofi), completed $151 million IPO Christian Kuhlen, MD General Counsel • General Counsel at Ignyta and Genoptix (acquired by Novartis),
executed multiple financings and M&A • Attorney at Cooley LLP Edna Chow Maneval, PhD • Previously SVP at Ignyta; clinical lead for entrectinib, led transition team through global filings SVP Clinical Development • VP of
Clinical Development at Seragon and Aragon, clinical lead for apalutamide • Led pivotal Phase 3 study in RCC for Sutent at Pfizer 4

Clinical Pipeline Focused on Advancement of ORIC-114 and ORIC-944 Lead
Lead Program Indication Identification Optimization IND Enabling Phase 1 Phase 2 Phase 3 Key Differentiation PRODUCT CANDIDATES NSCLC, Breast & ✓ CNS active ORIC-114 Phase 1b: ORIC-114 single agent Tumor agnostic ✓ Well tolerated
EGFR/HER2 exon 20 inhibitor ✓ Potential best-in-class ORIC-944 Phase 1b: ORIC-944 single agent Prostate Cancer drug properties PRC2 inhibitor OUT-LICENSING CANDIDATE ✓ Single agent activity ORIC-533 Phase 1b: ORIC-533 combination
ready✓ Clean safety profile Multiple Myeloma CD73 inhibitor ✓ Immune activation DISCOVERY RESEARCH PROGRAMS ORIC-613 Breast cancer✓ First-in-class potential PLK4 inhibitor Solid tumors Multiple programs targeting resistance
mechanisms Solid tumors 5

Substantial Progress in 2023: Well Positioned to Build Value in 2024 and
Beyond 2023 Accomplishments and Next Steps ✓ Phase 1b dose escalation data presented at ESMO 2023 demonstrated potential best-in-class profile, ORIC-114 with favorable safety and both systemic and CNS activity in heavily pre-treated NSCLC
patients EGFR/HER2 exon 20 inhibitor ✓ Initiating multiple dose expansion cohorts in 1H 2024 ✓ Phase 1b dose escalation data demonstrated potential best-in-class drug properties and favorable ORIC-944 safety, supporting advancement
into combination development in prostate cancer PRC2 inhibitor ✓ Initiating combination development with AR inhibitor(s) in 1H 2024 ✓ Phase 1b dose escalation data presented at ASH 2023 demonstrated favorable safety and clinical
ORIC-533 activity in heavily pre-treated multiple myeloma patients CD73 Inhibitor ✓ Pursuing strategic partnership for combination studies ✓ Presented preclinical data confirming therapeutic potential of highly selective PLK4
inhibitors as synthetic lethal for TRIM37 amplified breast cancer Discovery Research ✓ Advanced ORIC-613, a novel, highly selective PLK4 inhibitor, through IND enabling studies ✓ Strengthened balance sheet with $85 million financing
from healthcare specialist funds Corporate ✓ Extended cash runway into 2026 ORIC-114 and 944 rapidly advancing, with potential registrational studies for both programs expected to initiate in 2025 6

ORIC-114 Brain Penetrant EGFR/HER2 Exon 20 Inhibitor

ORIC-114 Is a Promising Candidate for Patients with Tumors Harboring
EGFR and HER2 Exon 20 Insertion Mutations, Including Those with Brain Metastases ORIC-114 Target Product Profile • Selectively targets EGFR and HER2 with high potency against exon 20 insertion mutations • Exquisite kinome selectivity
with limited potential Selective and Potent for off-target activity 800 600 • Significant tumor regression in multiple exon 20 400 insertion models 200 Promising Phase 1b Results 0 0 5 10 15 20 25 Days After Treatment • Superior
therapeutic index in vivo with improved efficacy and tolerability than competitor molecules ✓ Well tolerated safety profile Robust In Vivo Efficacy ✓ Systemic activity post-amivantamab ✓ CNS activity • High unbound (free)
brain exposures in vivo • Substantial tumor regression in intracranial efficacy studies Highly Brain Penetrant ORIC-114 is a potentially best-in-class EGFR and HER2 exon 20 inhibitor with excellent selectivity and brain penetrance 8 3 Mean
Tumor Volume (mm )

ORIC-114 Was Designed to Selectively Target EGFR and HER2 with High
Potency Against Exon 20 Insertion Mutations Kinome Selectivity Comparison CLN-081 Furmonertinib BLU-451* Mobocertinib ORIC-114 Off-target Wildtype (WT) Kinases Inhibited 80-100% at 1mM ORIC-114 CLN-081 Furmonertinib BLU-451 Mobocertinib 0 7
4 7* 7 ORIC-114 has demonstrated an exquisitely clean kinome panel, which is especially important for covalent inhibitors Source: Junttila et al. ESMO Poster (2023) and Murray et al. AACR Poster (2022). Note: ORIC-114,
mobocertinib, CLN-081, data conducted head-to-head in 468 kinases at 1µM. Top 10% shown. *BLU-451 data not conducted head-to-head in 409 kinases at 1µM. 9

ORIC-114 Demonstrates Potent In Vivo Activity in EGFR Exon 20 Insertion
Models In Vivo Efficacy – NSCLC EGFR Exon 20 Insertion Models EGFR Exon 20 insNPH EGFR Exon 20 insASV EGFR Exon 20 insG 3000 800 800 Vehicle Vehicle Vehicle ORIC-114 (4 mg/kg QD) ORIC-114 (4 mg/kg QD) ORIC-114 (4 mg/kg QD) 600 600 2000 400 400
1000 200 200 112% TGI 127% TGI 110% TGI 0 0 0 0 5 10 15 20 25 0 5 10 15 20 25 0 5 10 15 20 25 Days After Treatment Days After Treatment Days After Treatment ORIC-114 demonstrates potent tumor regression in multiple NSCLC EGFR exon 20 insertion
models without significant body weight loss Source: Junttila et al. AACR Poster (2021). 10 3 Mean Tumor Volume (mm ) 3 Mean Tumor Volume (mm ) 3 Mean Tumor Volume (mm )

Drugs Lacking CNS Activity Often Have Worse Clinical Outcomes in NSCLC
Case Study on NSCLC Targeted Therapy without CNS Activity: Mobocertinib • In mobocertinib’s phase 1/2 trial, ~35% of patients had CNS metastases at baseline Patients WITHOUT 8.1 CNS Metastases at Baseline • Patients with CNS
metastases at baseline had markedly worse outcomes ─ Brain was the first site of progression in 68% of patients with CNS metastases at baseline and in 38% of all patients Patients WITH 3.7 CNS Metastases at Baseline ─ ORR was 25% in
patients with CNS metastases at baseline compared to 43% in all patients 0.0 2.0 4.0 6.0 8.0 10.0 Median Progression Free Survival (Months) Approximately 35% of EGFR exon 20 NSCLC patients have CNS metastases at baseline and the brain is a frequent
site of progression in patients with and without CNS metastases at baseline, leading to shorter PFS with therapies lacking CNS activity Source: Janne et al. ASCO Presentation (2019) and Ramalingam et al. ASCO Poster (2021). 11

Superior Brain Penetration of ORIC-114 Differentiates from Comparator
Exon 20 Targeted Agents ORIC-114 Properties Allowed ORIC-114 Exhibits High Ratio of Free (Unbound) Optimization of Brain Exposure Brain/Plasma Exposure in Mice • Minimal pump engagement 10 ─ Key pumps that limit brain penetration, PGP
and BCRP drug transporters, have minimal impact on 1 ORIC-114 in cell assays • Suitable physicochemical properties 0.1 ─ LogP, LogD, TPSA, MW, HBD/HBA, pKa • High free unbound exposure in brain tissue 0.01 ─ Mouse Kp,uu 0.5
─ Dog Kp,uu 1.5 * * 0.001 ORIC-114 Mobocertinib CLN-081 BDTX-189 Osimertinib Extensive preclinical profiling demonstrates superior CNS properties of ORIC-114 versus competitors; Excellent free brain exposure across species for ORIC-114 as
exhibited by Kp,uu Source: Junttila et al. AACR Poster (2021), Junttila et al. AACR-NCI-EORTC Presentation (2021) and ORIC data on file. * Brain exposures were below quantification limit. 12 Free Brain/Plasma Ratio (@ 4 hr)

First-In-Human Phase 1b Study of ORIC-114 Phase 1b, Multicenter,
Open-Label Study Dose Expansion (Part II) Accelerated Approval Dose Escalation (Part I) All Patients +/- CNS mets Cohorts (Ph 2) EGFR ex20 NSCLC +/- CNS Key Eligibility naïve to EGFR ex20 therapy • Advanced solid tumors RP2D 1 ─
EGFR exon 20 EGFR ex20 NSCLC +/- CNS ORIC-114 ─ HER2 exon 20 post-amivantamab • Single agent ─ HER2+ • i3+3 design ─ EGFR atypical EGFR atypical mutated NSCLC +/- CNS • Active CNS • Oral QD/BID daily dosing
RP2D 2 Candidate metastases allowed RP2Ds • Prior EGFR exon 20 Selected HER2 ex20 NSCLC +/- CNS treatment allowed Primary endpoints: Part I: Safety and candidate RP2Ds; Part II: Dose expansion (RP2D selection) and ORR (per RECIST v1.1) Key
secondary endpoints: Part I: PK; Part II: Safety; DOR, CBR and PFS, including intracranial ORR/PFS Initial safety, PK/PD, and preliminary antitumor data from dose escalation (part I) presented at ESMO 2023 Note: ClinicalTrials.gov identifier:
NCT05315700. Dose expansion may include QD and BID dosing, fed/fasted dosing. RP2D = recommended Phase 2 dose 13 Screening / Enrollment

ORIC-114 Phase 1 Patient Disposition and Baseline Characteristics
Patient Disposition and Baseline Characteristics EGFR Ex20 HER2 Ex20 HER2+ Total (n=21) (n=24) (n=5) (N=50) 63 (31,80) 63 (25,86) 66 (48,68) 63 (25,86) Age, years, median(range) • 50 patients were treated with 10 (48) 11 (46) 3 (60) 24 (48)
Females, n (%) increasing doses of ORIC-114 ECOG performance score, n (%) • Of the NSCLC patients with 1 (5) 10 (42) 3 (60) 14 (28) 0 EGFR exon 20 20 (95) 14 (58) 2 (40) 36 (72) 1 12 (57) 16 (68) 3 (60) 31 (62) Non-smoker, n (%) ─
≥1 prior EGFR ex20: 81% 2 (1,6) 2 (0,7) 4 (1,7) 2 (0,7) Prior lines of therapies, median (min, max) ─ ≥2 prior EGFR ex20: 19% Prior therapies, n (%) 21 (100) 23 (96) 5 (100) 49 (98) Chemotherapy ─ CNS mets at baseline: 86% 18
(86) 1 (4) – 19 (38) EGFR targeted agents • Of the NSCLC patients with EGFR exon 20 targeted agents 17 (81) – – 17 (34) HER2 exon 20 15 (71) – – 15 (30) Amivantamab Mobocertinib 4 (19) – – 4 (8)
─ ≥1 prior HER2 agent: 30% Other (CLN-081, BLU-451) 2 (10) – – 2 (4) ─ CNS mets at baseline: 38% HER2 targeted agents – 7 (30) 3 (60) 10 (20) 18 (86) 9 (38) 1 (20) 28 (56) CNS metastases at baseline, n (%) Phase
1b enrolled heavily pretreated patients with exceptionally high rates of prior exon 20 targeted therapy and CNS metastases at baseline Note: All data as of the data cut-off on September 26, 2023. 14

ORIC-114 Has Been Generally Well Tolerated Despite More
Heavily-Pretreated Patients and Less Stringent Enrollment Criteria for Prior Therapy and CNS Disease Treatment Related Adverse Events Occurring in ≥10% of Patients <45 mg TDD 45 – 60 mg TDD ≥75 mg TDD Total (n=18) (n=23) (n=9)
(N=50) • Well tolerated safety profile Preferred Term, n (%) Gr1 Gr2 Gr3 ≥Gr4 Gr1 Gr2 Gr3 ≥Gr4 Gr1 Gr2 Gr3 ≥Gr4 All Grades with mostly Grade 1-2 Rash* 6 (33) 4 (22) – – 6 (26) 6 (26) – – 4 (44) 1 (11)
– – 27 (54) TRAEs Diarrhea 2 (11) 2 (11) – – 7 (30) 2 (9) 2 (9) – 2 (22) 2 (22) 1 (11) – 20 (40) • Minimal EGFR-wt related or Stomatitis 4 (22) 2 (11) – – 2 (9) 2 (9) 1 (4) – 2 (22) 2 (22)
– – 15 (30) other toxicities Paronychia 1 (6) 2 (11) – – 4 (17) 4 (17) – – 2 (22) 1 (11) – – 14 (28) • Low rates and severity of rash and diarrhea Pruritis 2 (11) – – – 4 (17) 2
(9) 1 (4) – 1 (11) 1 (11) – – 11 (22) ─ No Grade ≥3 rash Nausea 1 (6) – – – 2 (9) 2 (9) – – 1 (11) 1 (11) 1 (11) – 8 (16) ─ Low rate of Grade 3 Decreased appetite – 1 (6)
– – 5 (22) 1 (4) – – – – – – 7 (14) diarrhea (6%) Vomiting 2 (11) – – – 2 (9) – – – 1 (11) 1 (11) 1 (11) – 7 (14) • Infrequent dose reduction Dose
Reductions 2 (18) 3 (13) 3 (33) 8 (16) and discontinuations Dose Discontinuations 1 (9) 1 (4) – 2 (4) ORIC-114 was well tolerated with mainly Grade 1 and 2 adverse events and little evidence of off-target toxicities Note: All data as of the
data cut-off on September 26, 2023. * Rash includes the following terms: acne, dermatitis, dermatitis acneiform, eczema, hand dermatitis, and rash. TDD, total daily dose. TRAE, treatment related adverse event. 15

EGFR Exon 20: Tumor Regression Observed Across All Active ORIC-114
Doses Preliminary Activity (NSCLC patients with EGFR exon 20 and treated at ≥45 mg TDD) 60 40 20 0 -20 uPR Total Daily Dose -40 PR PR 90 mg -60 75 mg 60 mg -80 45 mg -100 CR Prior EGFR + + - - + + + + + + - + - + + exon 20 therapy CNS
Metastases + + + + + + - + - + + + + + + at Baseline Best CNS ND PD PD SD/PR PD PD ― SD/PR ― SD/PR SD/PR SD/PR SD/PR SD/PR CR Response 2 of 3 CNS 4 of 4 CNS lesions lesions resolved resolved Systemic and CNS activity observed in heavily
pretreated patients, including prior EGFR exon 20 therapy & active brain metastases Note: All data as of the data cut-off on September 26, 2023. ND: not done, SD/PR: Non-CR/Non-PD (RECIST 1.1), Response-evaluable: Dose level ≥45 mg TDD and
at least one post-baseline tumor assessment. 16 Best % Change in Target Lesions from Baseline

Confirmed Complete Intracranial and Systemic Response in Patient with
EGFR Exon 20 Mutated NSCLC and Active CNS Metastases Progressed on Prior EGFR Exon 20 Targeted Therapy • Patient: 55F with EGFR exon 20 mutated NSCLC • Prior therapy: Pemetrexed/cisplatin and amivantamab • Metastases
at baseline: Four active CNS non-target lesions ─ Previously untreated ─ No prior surgery ─ No prior radiation Baseline End of Cycle 2: Complete Response • ORIC-114 dose: 75 mg QD • Systemic response: Partial response
after Cycle 1 (60% reduction in all target and non-target lesions) followed by complete response at the end of Cycle 2 (100% reduction of all target and non-target lesions), subsequently confirmed • CNS response: Complete response after Cycle
1 (100% reduction of all 4 CNS lesions) confirmed after Cycle 2 • Grade ≥2 treatment-related AEs: Grade 2 mucositis and paronychia • Duration of treatment: Cycle 9 (ongoing) Baseline (1 out of 4 lesions shown) End of Cycle 1:
Complete Response ORIC-114 demonstrated single agent clinical activity in a key cancer and molecular subtype (i.e., NSCLC and EGFR exon 20) in a patient typically excluded from clinical trials (i.e., active brain metastases) and previously treated
with EGFR exon 20 therapy Note: All data as of the data cut-off on September 26, 2023. 17

ORIC-114 Is the Only EGFR Exon 20 Inhibitor to Demonstrate a Systemic
Complete Response and CNS Complete Response, Despite More Challenging Patients Comparison of Selected Eligibility Criteria, Baseline Characteristics, and Clinical Activity • EGFR exon 20 inhibitor clinical Amivantamab CLN-081 Sunvozertinib
Furmonertinib BLU-451 ORIC-114 studies typically EXCLUDE: Trial Phase 1 Phase 1 Phase 2 Phase 1 Phase 1 Phase 1 ─ Prior EGFR exon 20 treatment ENROLLMENT (1) ─ Untreated CNS metastases Prior EGFR ex20i Allowed No No No No Yes Yes •
ORIC-114 trial enrolled significantly % Prior EGFR ex20i 1% 4% 3% NR 75% 81% higher percentage of patients with Untreated CNS Mets Allowed No No No No Yes Yes prior EGFR exon 20 treatment and baseline CNS metastases % Baseline CNS Mets 22% 38% 32%
34% 58% 86% • Despite more challenging patients, CLINICAL ACTIVITY ORIC-114 demonstrated: Systemic Complete Response Yes No No No No Yes ─ Systemic complete response CNS Complete Response in No No No No No Yes (2) Untreated CNS Mets
─ CNS complete response in untreated CNS metastases ORR in EGFR ex20i Naive ~40% ~41% ~61% 42% TBD TBD 33% confirmed ─ Responses post-amivantamab Post-Amivantamab Response NA No Yes No No ORR (at 75 mg) Even while allowing patients with
prior exon 20 treatment and untreated brain metastases, ORIC-114 is the only EGFR exon 20 inhibitor to demonstrate a confirmed complete systemic response and confirmed complete CNS response Note: All data as of the data cut-off on September 26,
2023. Source: Park et al. J Clin Oncol (2021), Zhou et al. JAMA Oncology (2021), Piotrowska et al. J Clin Oncol (2023), Han et al. WCLC Presentation (2023), Wang et al. ASCO Presentation (2023), and Nguyen et al. ASCO Poster (2023). (1) Amivantamab
prohibited prior EGFR exon 20 treatment in dose expansion. CLN-081 allowed prior EGFR exon 20 treatment selectively during accelerated titration dose escalation only. (2) Treatment history for brain metastases not disclosed for BLU-451.
18

HER2 Exon 20: Tumor Regression Observed Across All Active ORIC-114
Doses Preliminary Activity (NSCLC patients with HER2 exon 20 and treated at ≥45 mg TDD) 60 40 20 0 -20 uPR uPR Total Daily Dose -40 PR 90 mg -60 PR 75 mg 60 mg -80 45 mg -100 PR Prior HER2 - + - - - - + - - - - + - therapy CNS Metastases + - -
+ - - - - - + + - - at Baseline Best CNS SD/PR ― ― ND ― ― ― ― ― SD/PR SD/PR ― ― Response Shrinkage of CNS lesions ORIC-114 demonstrated clinical activity in patients with HER2 exon 20 NSCLC,
including in patients with baseline brain metastases Note: All data as of the data cut-off on September 26, 2023. ND: not done, SD/PR: Non-CR/Non-PD (RECIST 1.1), Response-evaluable: Dose level ≥45 mg TDD and at least one post-baseline tumor
assessment. 19 Best % Change in Target Lesions from Baseline
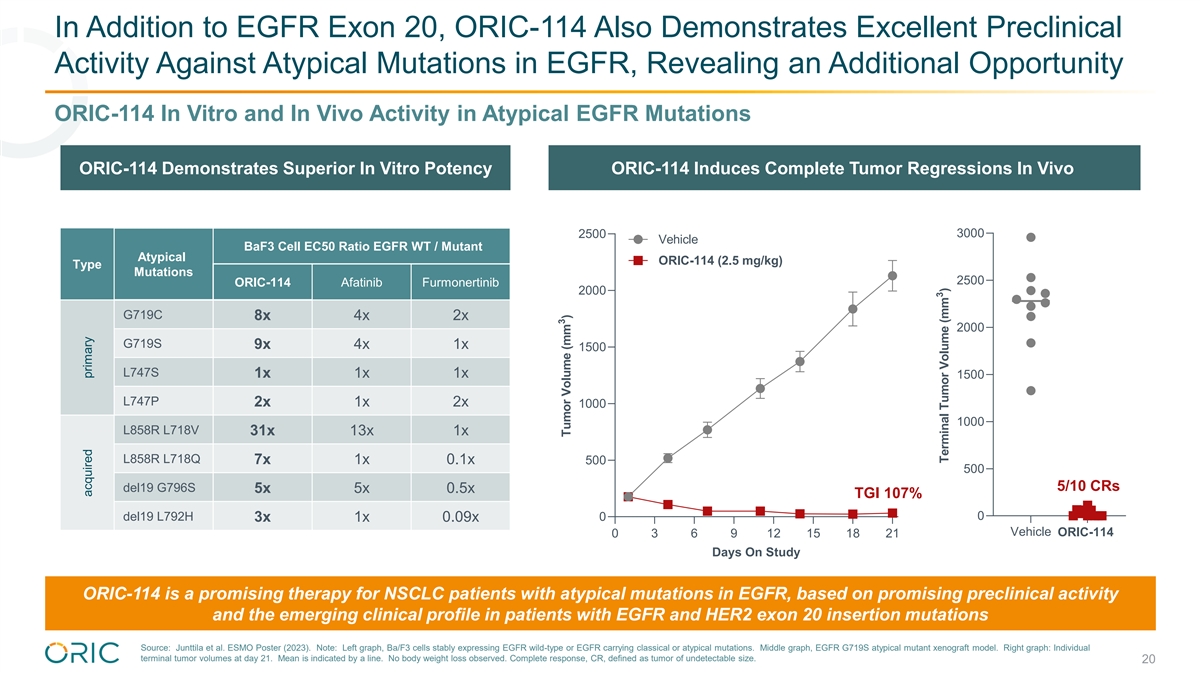
In Addition to EGFR Exon 20, ORIC-114 Also Demonstrates Excellent
Preclinical Activity Against Atypical Mutations in EGFR, Revealing an Additional Opportunity ORIC-114 In Vitro and In Vivo Activity in Atypical EGFR Mutations ORIC-114 Demonstrates Superior In Vitro Potency ORIC-114 Induces Complete Tumor
Regressions In Vivo 3000 2500 Vehicle BaF3 Cell EC50 Ratio EGFR WT / Mutant Atypical ORIC-114 (2.5 mg/kg) Type Mutations 2500 ORIC-114 Afatinib Furmonertinib 2000 G719C 8x 4x 2x 2000 G719S 9x 4x 1x 1500 L747S 1x 1x 1x 1500 L747P 2x 1x 2x 1000 1000
L858R L718V 31x 13x 1x L858R L718Q 7x 1x 0.1x 500 500 5/10 CRs del19 G796S 5x 5x 0.5x TGI 107% 0 del19 L792H 0 3x 1x 0.09x Vehicle ORIC-114 0 3 6 9 12 15 18 21 Days On Study ORIC-114 is a promising therapy for NSCLC patients with atypical mutations
in EGFR, based on promising preclinical activity and the emerging clinical profile in patients with EGFR and HER2 exon 20 insertion mutations Source: Junttila et al. ESMO Poster (2023). Note: Left graph, Ba/F3 cells stably expressing EGFR wild-type
or EGFR carrying classical or atypical mutations. Middle graph, EGFR G719S atypical mutant xenograft model. Right graph: Individual terminal tumor volumes at day 21. Mean is indicated by a line. No body weight loss observed. Complete response, CR,
defined as tumor of undetectable size. 20 acquired primary 3 Tumor Volume (mm ) 3 Terminal Tumor Volume (mm )

ORIC-114 Planned Next Steps and Potential Registrational Path(s) 2024
2025 - 2026 2027 ❑ EGFR exon 20 inhibitor-naïve Phase 1b Dose ❑ EGFR atypical mutations Expansion ❑ HER2 exon 20 EGFR exon 20, naïve to prior exon 20 EGFR exon 20, post-amivantamab Multiple Potential Potential Phase 2
NDA Filings in 2027 Accelerated Approval for Accelerated Cohorts in NSCLC EGFR atypical mutations Approvals HER2 exon 20 Updated Phase 1b data expected in 1H 2025; Potential for multiple accelerated registrational cohorts initiating in 2025
21

ORIC-114 Is Pursuing a Significant Commercial Opportunity Across
Multiple Patient Populations that Do Not Have CNS Active Agents Approved or in Late-Stage Development Estimated US Prevalence of Exon 20 Insertions (% of NSCLC) 10 14.0% .0% ORIC-114 Target Population: 12.5% 6.5% of NSCLC 18 2..0 0% % 2.9% 6.0% 4.4%
1.5% 4.0% 2.1% 2.0% 1.5% 0.0% EGFR Exon 20 HER2 Exon 20 Atypical EGFR RET ALK EGFR Approved Agents with Pralsetinib/Selpercatinib Alectinib Osimertinib CNS Activity: Worldwide Annualized ─ ─ ─ $325m (+54% YoY) $1,700m (+1% YoY)
$6,000m (+7% YoY) 2Q23 Estimated Sales: The commercial opportunity for ORIC-114 may represent up to 6.5% of NSCLC (>12,500 patients) in the US annually Source: American Cancer Society Cancer Facts & Figures 2023, Gainor et al. Clin Cancer Res
(2013), Hirsch et al. Lancet (2017), Rosen et al. Clin Cancer Res (2021), Heymach et al. WCLC Presentation (2018) and Robichaux et al. Nature (2021). AstraZeneca, Roche and Lilly corporate filings. Note: Worldwide annualized 2Q23 estimated sales
calculated using reported 2Q23 sales and adjusted for an annual run rate. 22 Estimated % of NSCLC in the US

ORIC-944 Allosteric PRC2 Inhibitor

ORIC-944 Is a Promising Next-Generation PRC2 Inhibitor Focused on
Patients with Prostate Cancer ORIC-944 Target Product Profile • Allosteric inhibitor of PRC2 by selectively targeting EED • Picomolar biochemical potency Selective and Potent Promising Phase 1b • Significant single agent activity
demonstrated in Results treatment resistant prostate cancer models ✓ Best-in-class drug • ORIC-944 appears more effective than EZH2 inhibitors in Robust In Vivo Efficacy properties preclinical models ✓ Robust target engagement
✓ Well tolerated safety profile • Approved and other PRC2 inhibitors in development appear to be limited by poor drug properties Best-in-Class Drug • ORIC-944 designed for improved drug properties over Properties other PRC2
inhibitors ORIC-944 is a potential best-in-class PRC2 inhibitor with superior drug properties suitable for combination development in prostate cancer 24

PRC2 Plays Pivotal Role in Transcriptional Regulation and Cancer PRC2
Function PRC2 Background PRC2 • Two druggable subunits: – EED: responsible for histone binding; target of ORIC-944 EZH2 – EZH2: responsible for histone methylation; target of first- EED generation inhibitors • Dysregulation
of PRC2 linked to several cancers SUZ12 – Decreased expression of target genes associated with poor Tri-methylation (1) prognosis in prostate cancer of H3K27 • First-generation inhibitors, designed to inhibit EZH2, have demonstrated
promising clinical activity – Approved for epithelioid sarcoma and follicular lymphoma Tumorigenesis – Emerging potential in prostate cancer Gene silencing Cell fate / differentiation PRC2 is a validated oncogenic target across several
cancers with promising therapeutic potential in prostate cancer Note: EZH1, enhance of zeste homolog 1. EZH2, enhance of zeste homolog 2. EED, embryonic ectoderm development. SUZ12, suppressor of zeste 12. H3K27, histone H3 at lysine 27. (1) Yu et
al. Cancer Res. (2007). 25

ORIC-944 Targets the EED Subunit of PRC2 and Has Demonstrated Superior
Single Agent In Vivo Efficacy and Favorable Drug Properties EED Inhibition May Improve Upon EZH2 Inhibitors ORIC-944 Induces Complete Regression in DLBCL Model 1250 • ORIC-944 allosterically inhibits PRC2 by targeting EED • Allosteric
inhibition of PRC2 through EED may address 1000 Vehicle limitations of EZH2 inhibitors (1) – Active against EZH2 innate resistant PRC2 mutants 750 – Prevent acquired resistance through secondary (2) mutations in EZH2 500 (3) –
Inhibit compensatory bypass activity of EZH1 Tazemetostat • ORIC-944 is associated with improved drug properties 250 (200 mg/kg BID) (4) over other PRC2 inhibitors ORIC-944 • ORIC-944 appears more effective than EZH2 inhibitors (200
mg/kg QD) 0 0 10 20 30 40 50 in preclinical models Days After Treatment Allosteric PRC2 inhibition through EED provides many potential benefits over EZH2; Notably, ORIC-944 has improved drug properties over other PRC2 inhibitors Source: Daemen et
al. AACR Poster (2021). (1) Qi et al. Nat Chem Biol (2017). (2) Bisserier et al. Blood (2018). (3) Shen et al. Mol Cell (2008) and Honma et al. Cancer Sci (2017). (4) Italiano et al. Lancet Oncol (2018), Harb et al. TAT (2018) and Yap et al. Clin
Cancer Res (2019). Note: DLBCL, diffuse large B-cell lymphoma. Right graft: KARPAS-422 xenograft model. 26 3 Tumor Volume (mm )

ORIC-944 Demonstrated Strong Single-Agent Activity in Prostate Cancer
Models In Vivo Efficacy – Prostate Cancer Models Androgen-Insensitive Prostate Cancer Enzalutamide-Resistant AR-v7+ Prostate Cancer 2000 1000 Vehicle 1500 750 Vehicle Enzalutamide 1000 500 Enzalutamide **** **** ORIC-944 500 250 ORIC-944 79%
tumor growth inhibition 86% tumor growth inhibition 0 0 0 10 20 30 0 10 20 30 Days After Treatment Days After Treatment Based on In vivo efficacy observed in multiple prostate cancer models and improved drug properties, ORIC-944 is positioned as a
potential best-in-class PRC2 inhibitor for prostate cancer Source: ORIC data and Daemen et al. AACR Poster (2021). Note: ORIC-944 dose used was 200 mg/kg QD. Enzalutamide dose used was 30 mg/kg QD. ****p < 0.0001. Left graph: C4-2 xenograft
model. Right graph: 22Rv1 xenograft model. 27 3 Tumor Volume (mm ) 3 Tumor Volume (mm )

PRC2 Epigenetic Dysregulation Plays a Key Mechanistic Role During the
Progressive Reprogramming of Prostate Cancers Treated with AR Inhibitors AR Independent Prostate Cancer AR Dependent Prostate Cancer • Prostate cancer cells evade therapies by cellular reprogramming to an AR independent state • PRC2
inhibition can Castration sensitive Castration resistant Heterogeneous Lineage change reverse this process, such that prostate cancer cells regain AR dependency AR-directed therapeutics • Mechanistic rationale supports combination of PRC2
inhibitors with AR Luminal cell (AR+) inhibitors PRC2 inhibitors Basal cell (No AR) Neuroendocrine cell (No AR) Therapeutic potential of PRC2 inhibitors in prostate cancer is maximized in combination with AR inhibitors Source: Mu et al. Science
(2017), Dardenne et al. Cancer Cell (2016), Davies et al. Nat Cell Biol (2021), Nouruzi et al. Nat Commun (2022), and Goel et al. Semin Cancer Bio (2022). 28

ORIC-944 Synergizes with AR Inhibitors in Preclinical Prostate Cancer
Models Combination Potential of PRC2 and AR Inhibition Preclinical Synergy Assessment Synergy Score Results 10 and above = Synergy ORIC-944 PF-1497 Synergistic • Synergy observed with ORIC-944 combination with + enzalutamide + enzalutamide
Analysis enzalutamide in preclinical prostate cancer model ─ Cellular growth assay over 14 days Bliss 10.6 9.9 ─ Dose-ranging concentrations of enzalutamide and PRC2 inhibitor, alone and in combination ─ Synergy scoring via
multiple models Loewe 15.8 14.1 • Synergy also demonstrated with ORIC-944 in transcriptional based analysis, in combination with other AR inhibitors, and in additional prostate cancer HSA 16.7 15.4 cell lines -10 and below = Antagonistic
ORIC-944 synergizes with AR inhibitors in prostate cancer models, providing rationale for clinical development Source: Data in C4-2 prostate cancer cells shown. 29 Synergy Score Interpretation

Pfizer Phase 1 Data Clinically Validates Synergy of PRC2 Inhibitor and
AR Inhibitor in Prostate Cancer Updated PF-06821497 Phase 1 Data in Prostate Cancer (1Q23 Pfizer Earnings Call) Early rPFS data are encouraging and notably longer than historical controls In the control arm of the CARD study, rPFS for XTANDI alone
was 4.8 months in XTANDI- naïve patients These results, in combination with emerging objective response rate and PSA50 response, are supportive of the contribution of our EZH2 inhibitor candidate in driving these responses ─ Mikael
Dolsten, CSO and President, Worldwide Research, Development and Medical Durable antitumor activity was observed in both XTANDI naïve and experienced patients with mCRPC, both of which are notably longer than historical controls – Phase 2
randomized data expected in 2024 Source: Pfizer first quarter 2023 earning call on May 2, 2023. 30
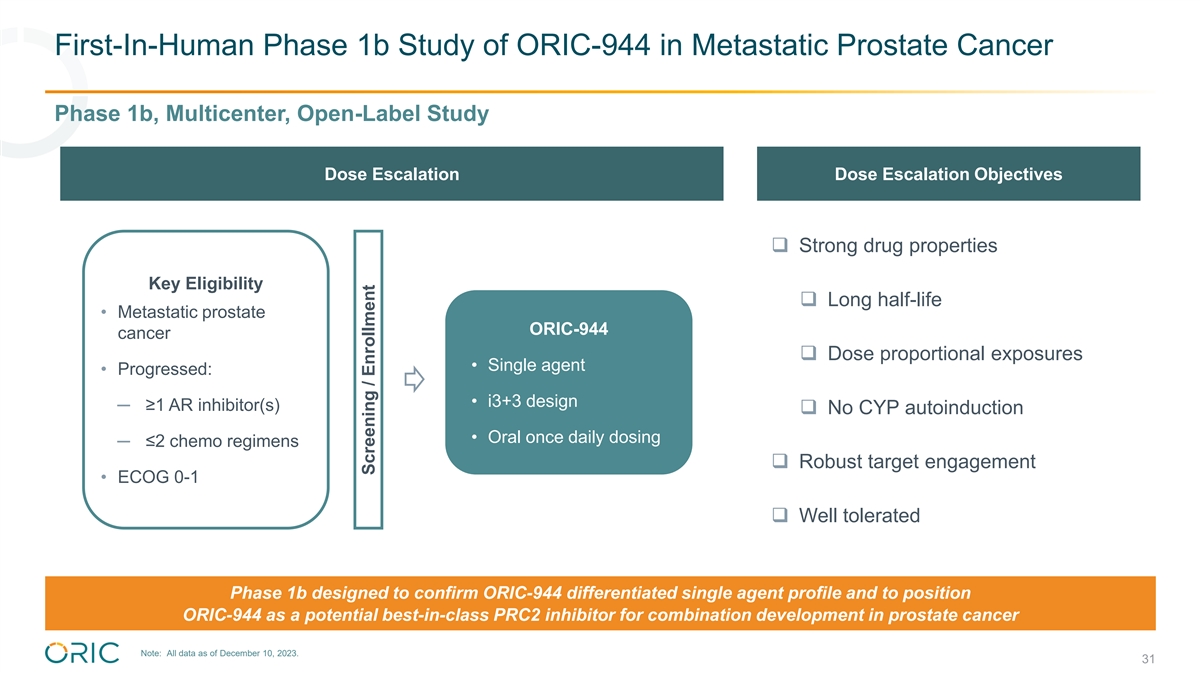
First-In-Human Phase 1b Study of ORIC-944 in Metastatic Prostate Cancer
Phase 1b, Multicenter, Open-Label Study Dose Escalation Dose Escalation Objectives ❑ Strong drug properties Key Eligibility ❑ Long half-life • Metastatic prostate ORIC-944 cancer ❑ Dose proportional exposures •
Single agent • Progressed: • i3+3 design ─ ≥1 AR inhibitor(s) ❑ No CYP autoinduction • Oral once daily dosing ─ ≤2 chemo regimens ❑ Robust target engagement • ECOG 0-1 ❑ Well
tolerated Phase 1b designed to confirm ORIC-944 differentiated single agent profile and to position ORIC-944 as a potential best-in-class PRC2 inhibitor for combination development in prostate cancer Note: All data as of December 10, 2023. 31
Screening / Enrollment

ORIC-944 Has Demonstrated a Potential Best-in-Class Pharmacokinetic
Profile Preliminary Phase 1b Pharmacokinetic Data Clinical Half-Life Comparison Key Takeaways 15 • Excellent pharmacokinetic profile observed to date ─ Increased exposure with dose level >10 hours ─ Low inter-patient variability
10 • No signs of CYP autoinduction that is observed with first-generation PRC2 inhibitors 5 • Clinical half-life consistent with preclinical prediction <4 hours 3 hours of >10 hours, which is superior to other PRC2 inhibitors and
supports QD dosing • Exposures at ≥600 mg QD exceed target Cmin that 0 Tazemetostat PF-1497 ORIC-944 provides 90% TGI in preclinical in vivo prostate Lack of CYP cancer models û✓✓ Autoinduction Dose exploration
continues with favorable plasma half-life and exposures consistent with best-in-class drug properties Note: All data as of December 10, 2023. Source: Tazemetostat half-life from FDA label. PF-06821497 half-life estimated from Schweizer et al. ESMO
Poster (2022). 32 Clinical Half-life (hours)

ORIC-944 Has Demonstrated Robust and Consistent Target Engagement
Preliminary Phase 1b Pharmacodynamic Data Inhibition of PRC2 Activity Key Takeaways (% H3K27me3 Reduction in Monocytes) Once Daily Dosing (QD) 200 mg 400 mg 600 mg 900 mg • Robust target engagement demonstrated with once- 0 daily monotherapy
dosing -25 • Maximal decrease (≥75%) in H3K27me3 in monocytes from peripheral blood samples achieved across multiple dose levels, starting as low as 200 mg QD -50 • Low inter-patient variability observed -75 -100 ORIC-944 has
demonstrated promising pharmacodynamic data, indicating strong target engagement Note: All data as of December 10, 2023. Note: % H3K27me3 inhibition in monocytes from Phase 1b patients shown on plot. Samples collected at cycle 1 day 15, or at cycle
1 day 22 for 2 patients at 400 mg QD. H3K27me3, trimethylation of lysine 27 of histone H3. 33 % Change from Baseline of H3K27me3/H3 at C1D15 (Mean± SEM)

ORIC-944 Is Advancing into Combination Development Based on Phase 1
Results Phase 1b, Multicenter, Open-Label Study Initial Phase 1b Results Phase 1b Dose Expansion • Potential best-in-class drug properties with half-life Key Eligibility >10 hours supporting once-daily dosing • Metastatic prostate
ORIC-944 cancer • Robust target engagement demonstrated with • Combination with AR • Progressed on maximal decrease (≥75%) in H3K27me3 in inhibitor(s) abiraterone (no prior nd 2 generation AR monocytes from peripheral blood
samples • i3+3 design inhibitor) • Oral once daily dosing • Well tolerated to date • Up to 1 prior chemo • ECOG 0-1 ─ Only grade 1 and 2 TRAEs at dose levels less than 900 mg QD Primary endpoints: Safety and
recommended Phase 2 dose Key secondary endpoints: Safety; DOR, CBR and PFS Exploratory endpoints: H3K27 trimethylation, PRC2 target gene expression, PSA, and genomics ORIC-944 demonstrated potential best-in-class drug properties with favorable
safety and strong PK profile supporting QD dosing; Combination study with AR inhibitor(s) to be initiated in 1H 2024 Note: All data as of December 10, 2023. 34 Screening / Enrollment
ORIC-533 Orally Bioavailable Small Molecule Inhibitor of
CD73

ORIC-533 Is a Potential Best-in-Class Inhibitor of CD73 and
First-in-Class for the Treatment of Multiple Myeloma ORIC-533 Target Product Profile • Adenosine is immunosuppressive and impairs antitumor immunity • CD73 reverses immunosuppression in preclinical studies CD73 Has Significant •
CD73 inhibition has demonstrated positive randomized phase 2 data Therapeutic Potential in NSCLC in combination with PD-L1 inhibition in Oncology Promising Phase 1b Results • More potent than benchmark inhibitors in T cell activation assays
✓ Once daily oral dosing • Orally administered small molecule provides benefits over antibodies ORIC-533 Is a Potential (ease of administration and increased tumor penetration) ✓ Clean safety profile Best-in-Class • Clean
safety profile observed in preclinical toxicology studies ✓ Dose dependent CD73 Inhibitor immune activation ✓ Clinical activity as • CD73 and adenosine role in multiple myeloma supported by single agent in research of Dr. Kenneth
Anderson lab at Dana Farber Cancer heavily-pretreated Institute ORIC-533 Is multiple myeloma First-in-Class for • Activity demonstrated in ex vivo bone marrow assays from patients Multiple Myeloma with relapsed/refractory multiple myeloma
ORIC-533 demonstrated immune activation with an exceptionally clean safety profile, which translated into the first single agent activity of any CD73 inhibitor in clinic; well positioned for combination studies in multiple myeloma 36

Initial First-In-Human Phase 1b Results of ORIC-533 in r/r Multiple
Myeloma Were Presented at ASH 2023 Phase 1b, Multicenter, Open-Label Study Phase 1b Dose Escalation Initial Phase 1b Results ✓ Clinical half-life of ~24 hours supports QD dosing Key Eligibility ✓ Well tolerated safety profile with no
Grade ≥3 TRAEs • r/r multiple myeloma ORIC-533 • Refractory to or ✓ Complete/substantial inhibition of CD73 activity in serum ineligible for treatment • Single agent and bone marrow regimens known to • i3+3
design provide clinical benefit ✓ Evidence of immune modulation of CD8+ T cells and NK • Oral once daily dosing (i.e., triple-class+ cells refractory) • ECOG 0-2 ✓ Meaningful reductions in sBCMA levels, suggestive of
antimyeloma activity Primary endpoints: Safety and recommended Phase 2 dose ✓ Preliminary evidence of clinical antimyeloma activity, Key secondary endpoints: PK including reductions in paraprotein, demonstrated in (1) multiple patients with
r/r multiple myeloma Exploratory endpoints: Exploratory biomarkers Phase 1b remains ongoing as a monotherapy to select provisional RP2D for combination development; Strategic partnership being pursued to enable combination studies (1) Exploratory
biomarker analyses include CD73 enzymatic function, and immune cell and cytokine profiling. Note: r/r, relapsed/refractory. NK, natural killer. sBCMA, soluble B-cell maturation antigen. 37 Screening / Enrollment

ORIC-613 Highly Selective PLK4 Inhibitor

ORIC Is Developing Small Molecule Inhibitors of PLK4 Targeting
TRIM37-Amplified Breast Cancer Via Synthetic Lethality PLK4 Inhibition Is Synthetically Lethal to ORIC Small Molecule Inhibitor of PLK4 Tumor Cells with TRIM37 Amplifications Discovery and Development Rationale Normal Cell • Polo-like kinase 4
(PLK4) is a serine/threonine protein kinase that controls centrosome duplication during cell division Reversible PLK4 + Cell Cycle = Inhibition Arrest • Cells with TRIM37 amplification require PLK4 function for growth and survival TRIM37
Amplified Cell ─ Provides opportunity for synthetic lethal targeting Mitotic • TRIM37 amplifications occur in breast cancer (~20%) PLK4 Catastrophe = + Inhibition and neuroblastoma (~55%), and have been and Cell Death associated with
early relapse and poor prognosis Mother centriole Daughter centriole Pericentriolar Material Targeting TRIM37 amplified cancers with a potent and selective PLK4 inhibitor is a potential first-in-class opportunity Source: Meitinger et al. Nature
(2020), Yeow et al. Nature (2020), Sinclair et al. Breast Cancer Res Treat (2003) and Bown et al. N Engl J Med (1999). 39

ORIC Small Molecule Inhibitors of PLK4 Are Highly Potent and Selective,
and Demonstrate Single Agent Activity In Vivo ORIC PLK4 Inhibitors Are Potent and Selective ORIC PLK4 Inhibitors Demonstrate Single Agent with Targeted Activity in TRIM37 Amplified Cell Lines Activity in TRIM37 Amplified Xenograft Model 1200 ORIC
PLK4 Inhibitor ORIC PLK4 Inhibitor ORIC PLK4 Inhibitor Vehicle (Compound Y) (Compound X) (Compound Z) Compound Z BID 1000 100000 100000 800 600 10000 10000 400 200 100% TGI 1000 1000 0 0 3 6 9 12 15 18 21 Days On Study 100 100 High Low High Low 20
TRIM37 TRIM37 10 0 ORIC PLK4 Inhibitors -10 Compound X Compound Y Compound Z -20 0 3 6 9 12 15 18 21 PLK4 Biochemical IC (nM) 0.43 1.58 1.79 50 Days On Study ORIC PLK4 inhibitors are highly selective and demonstrate strong single agent antitumor
activity in TRIM37 amplified xenografts; Advanced novel development candidate, ORIC-613, through IND enabling studies Source: Edgar et al. AACR Poster (2022). Left graphs: Kinome profile at 1 μM. Cell panel consists of breast cancer and
neuroblastoma cell lines. Right graphs: oral dosing of ORIC PLK4 inhibitor in CHP-134 neuroblastoma xenograft model. 40 IC (nM) 50 3 % Body Weight Change Tumor Volume (mm )

Key Takeaways

Clinical Pipeline Focused on Advancement of ORIC-114 and ORIC-944 Lead
Lead Program Indication Identification Optimization IND Enabling Phase 1 Phase 2 Phase 3 Key Differentiation PRODUCT CANDIDATES NSCLC, Breast & ✓ CNS active ORIC-114 Phase 1b: ORIC-114 single agent Tumor agnostic ✓ Well tolerated
EGFR/HER2 exon 20 inhibitor ✓ Potential best-in-class ORIC-944 Phase 1b: ORIC-944 single agent Prostate Cancer drug properties PRC2 inhibitor OUT-LICENSING CANDIDATE ✓ Single agent activity ORIC-533 Phase 1b: ORIC-533 combination
ready✓ Clean safety profile Multiple Myeloma CD73 inhibitor ✓ Immune activation DISCOVERY RESEARCH PROGRAMS ORIC-613 Breast cancer✓ First-in-class potential PLK4 inhibitor Solid tumors Multiple programs targeting resistance
mechanisms Solid tumors 42

ORIC Pharmaceuticals: Dedicated to Overcoming Resistance In Cancer
• Two potential best-in-class programs advancing towards pivotal studies Broad Pipeline of Potential First-in-Class and Best-in-Class Programs • Additional preclinical programs targeting novel and validated targets Precision Oncology
Expertise Enables • Rapid timelines enabled by biomarker-driven, patient-selected clinical Accelerated Clinical Timelines trials and translational expertise • Track record of building pipeline via internal R&D and business
development Dual Engines for Pipeline Expansion • Targeting one new IND candidate every 18 months • Heritage of discovering and developing multiple approved oncology medicines at Experienced Management Team Ignyta, Medivation, Aragon and
Genentech (1) Strong Financial Position • Cash and investments of $235 million expected to fund company into 2026 • ORIC-944 initiation of combination study with AR inhibitor(s): 1H 2024 • ORIC-944 program update: mid-2024
Anticipated Milestones • ORIC-114 initiation of dose expansion in multiple cohorts: 1H 2024 • ORIC-114 updated Phase 1b data: 1H 2025 (1) Approximate unaudited balance as of December 31, 2023. 43
v3.23.4
| X |
- DefinitionBoolean flag that is true when the XBRL content amends previously-filed or accepted submission.
| Name: |
dei_AmendmentFlag |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionFor the EDGAR submission types of Form 8-K: the date of the report, the date of the earliest event reported; for the EDGAR submission types of Form N-1A: the filing date; for all other submission types: the end of the reporting or transition period. The format of the date is YYYY-MM-DD.
| Name: |
dei_DocumentPeriodEndDate |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:dateItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe type of document being provided (such as 10-K, 10-Q, 485BPOS, etc). The document type is limited to the same value as the supporting SEC submission type, or the word 'Other'.
| Name: |
dei_DocumentType |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:submissionTypeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 1 such as Attn, Building Name, Street Name
| Name: |
dei_EntityAddressAddressLine1 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 2 such as Street or Suite number
| Name: |
dei_EntityAddressAddressLine2 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- Definition
+ References
+ Details
| Name: |
dei_EntityAddressCityOrTown |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCode for the postal or zip code
| Name: |
dei_EntityAddressPostalZipCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the state or province.
| Name: |
dei_EntityAddressStateOrProvince |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:stateOrProvinceItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionA unique 10-digit SEC-issued value to identify entities that have filed disclosures with the SEC. It is commonly abbreviated as CIK. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityCentralIndexKey |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:centralIndexKeyItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionIndicate if registrant meets the emerging growth company criteria. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityEmergingGrowthCompany |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCommission file number. The field allows up to 17 characters. The prefix may contain 1-3 digits, the sequence number may contain 1-8 digits, the optional suffix may contain 1-4 characters, and the fields are separated with a hyphen.
| Name: |
dei_EntityFileNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:fileNumberItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTwo-character EDGAR code representing the state or country of incorporation.
| Name: |
dei_EntityIncorporationStateCountryCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarStateCountryItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe exact name of the entity filing the report as specified in its charter, which is required by forms filed with the SEC. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityRegistrantName |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe Tax Identification Number (TIN), also known as an Employer Identification Number (EIN), is a unique 9-digit value assigned by the IRS. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityTaxIdentificationNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:employerIdItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionLocal phone number for entity.
| Name: |
dei_LocalPhoneNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 13e
-Subsection 4c
| Name: |
dei_PreCommencementIssuerTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 14d
-Subsection 2b
| Name: |
dei_PreCommencementTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTitle of a 12(b) registered security. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b
| Name: |
dei_Security12bTitle |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:securityTitleItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the Exchange on which a security is registered. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection d1-1
| Name: |
dei_SecurityExchangeName |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarExchangeCodeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as soliciting material pursuant to Rule 14a-12 under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Section 14a
-Number 240
-Subsection 12
| Name: |
dei_SolicitingMaterial |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTrading symbol of an instrument as listed on an exchange.
| Name: |
dei_TradingSymbol |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:tradingSymbolItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as written communications pursuant to Rule 425 under the Securities Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Securities Act
-Number 230
-Section 425
| Name: |
dei_WrittenCommunications |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
Oric Pharmaceuticals (NASDAQ:ORIC)
Historical Stock Chart
From Apr 2024 to May 2024

Oric Pharmaceuticals (NASDAQ:ORIC)
Historical Stock Chart
From May 2023 to May 2024
